Leah Grinshpun, Charlotte Abiezzi, Aliyah Carson, Vardan Dagstanyan, Sihye Edwards, Katarina Harrelson, Anita Ho, Aaron Lee, Kevin Ong, Vanessa Phan, Menka Webster, Taylor Willis, Dr. Jennifer Poast, Dr. Janelle Pieros, Dr. Steven Ritter, Ms. Kate Whelihan, Dr. Joy Lewis
Introduction
Adverse Childhood Events (ACEs) are abuse, neglect, and household challenges faced in the first 18 years of life and have been shown to be highly associated with poor health outcomes (Figure 1). The State of California has put forth a campaign to recognize, investigate, and address the effects of ACEs on lifelong health with a strong focus on mindfulness. The top diagnoses at San Ysidro Health (SYH) – obesity, anxiety, depression, hypertension, and diabetes – have been shown to positively correlate with ACE scores. In conjunction with the statewide campaign, SYH has created an ACE Screening Taskforce and initiated an effort to document ACE scores for all patients. Providers offer high-scoring patients behavioral health referrals, but long wait times make a point-of-care (POC) intervention necessary. Here, we aimed to identify and address toxic stress related to ACEs among adult patients at SYH. We propose a method to bring mindfulness techniques directly to patients that they can practice independently while waiting for mental health services.
METHODS
We began by conducting a statistical analysis of previously documented ACE scores and prevalence of depression, anxiety, obesity, hypertension, and DMI/II to establish a relationship between ACEs and health outcomes among adult patients at SYH.
Next, a workflow was developed to provide patients with a POC mindfulness intervention. Patients who completed ACE screenings during their visit were shown one of four mindfulness videos and subsequently asked to complete a survey that included personal demographics, perspectives on ACEs and mental health, and feedback on the videos. Patients were also provided with an informational sheet including a QR code (Figure 2) allowing them to continue to use the resource outside of the clinic, easily and free of cost.
A Plan-Do-Check-Act (PDCA) model was used to introduce and optimize the workflow at the one of SYH’s largest clinics – Chula Vista Medical Plaza (CVMP; Figure 3). Our protocol relied heavily on the CVMP’s existing ACE screening practices. We learned that there was a high rate of variability in terms of adherence to the SYH screening protocol. Therefore, we first helped to put in place a consistent practice of screening patients for ACEs before the intervention could be incorporated into the workflow.
Results
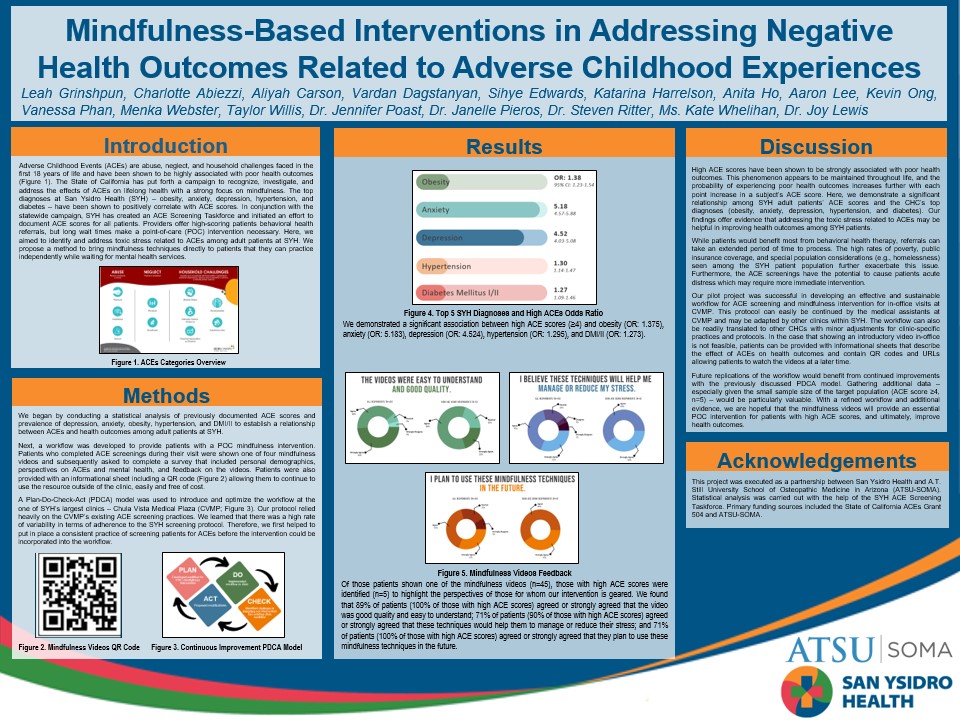
Of those patients shown one of the mindfulness videos (n=45), those with high ACE scores were identified (n=5) to highlight the perspectives of those for whom our intervention is geared. We found that 89% of patients (100% of those with high ACE scores) agreed or strongly agreed that the video was good quality and easy to understand; 71% of patients (90% of those with high ACE scores) agreed or strongly agreed that these techniques would help them to manage or reduce their stress; and 71% of patients (100% of those with high ACE scores) agreed or strongly agreed that they plan to use these mindfulness techniques in the future.
DISCUSSION
High ACE scores have been shown to be strongly associated with poor health outcomes. This phenomenon appears to be maintained throughout life, and the probability of experiencing poor health outcomes increases further with each point increase in a subject’s ACE score. Here, we demonstrate a significant relationship among SYH adult patients’ ACE scores and the CHC’s top diagnoses (obesity, anxiety, depression, hypertension, and diabetes). Our findings offer evidence that addressing the toxic stress related to ACEs may be helpful in improving health outcomes among SYH patients.
While patients would benefit most from behavioral health therapy, referrals can take an extended period of time to process. The high rates of poverty, public insurance coverage, and special population considerations (e.g., homelessness) seen among the SYH patient population further exacerbate this issue. Furthermore, the ACE screenings have the potential to cause patients acute distress which may require more immediate intervention.
Our pilot project was successful in developing an effective and sustainable workflow for ACE screening and mindfulness intervention for in-office visits at CVMP. This protocol can easily be continued by the medical assistants at CVMP and may be adapted by other clinics within SYH. The workflow can also be readily translated to other CHCs with minor adjustments for clinic-specific practices and protocols. In the case that showing an introductory video in-office is not feasible, patients can be provided with informational sheets that describe the effect of ACEs on health outcomes and contain QR codes and URLs allowing patients to watch the videos at a later time.
Future replications of the workflow would benefit from continued improvements with the previously discussed PDCA model. Gathering additional data – especially given the small sample size of the target population (ACE score ≥4, n=5) – would be particularly valuable. With a refined workflow and additional evidence, we are hopeful that the mindfulness videos will provide an essential POC intervention for patients with high ACE scores, and ultimately, improve health outcomes.
ACKNOWLEDGEMENTS
This project was executed as a partnership between San Ysidro Health and A.T. Still University School of Osteopathic Medicine in Arizona (ATSU-SOMA). Statistical analysis was carried out with the help of the SYH ACE Screening Taskforce. Primary funding sources included the State of California ACEs Grant 504 and ATSU-SOMA.