Improving Community Health Through Targeting Sodium Consumption
Can Community Health Centers Play a Role?
When you attend SOMA, you will make a difference in serving communities in need. After the first year of didactic learning, you will gain hands-on experience with patients in community clinics around the country. In fact, we are the only medical school that partners with the National Association of Community Health Centers to provide experiential learning to our medical students.
Service is at the heart of our mission and culture. At SOMA, you are not just earning a Doctor of Osteopathic Medicine. You are earning a place in the broader A.T. Still University educational and professional community as a doctor with a commitment to service and high ethical responsibility. Not only do you have access to the educational resources and innovative curriculum to become a remarkable osteopathic practitioner, but you also participate in extensive service-oriented training in communities that enables you to embark on a lifelong mission to make a difference.
Research Objectives
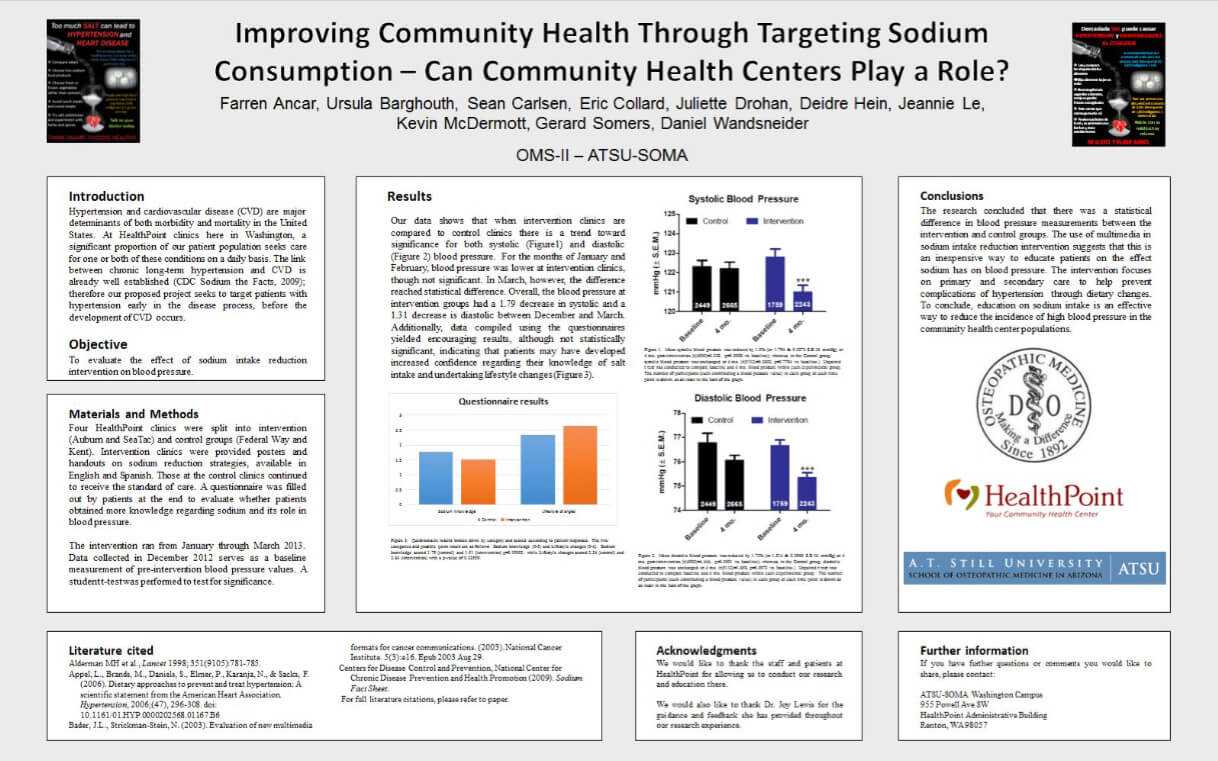
To evaluate the effect of a community health center based sodium intake reduction intervention on patient systolic and diastolic blood pressure.
Study Design/Methods
Four HealthPoint clinics were split into intervention and control groups over the period of January to March 2013. Intervention clinics were provided posters and handouts on sodium reduction strategies. Control clinic patients continued to receive the usual standard of care for hypertension management. Systolic and diastolic blood pressure data for all adults 18 and older who received care during the study period was collected using electronic medical records. Patients completed a questionnaire at the end of the study to assess patient knowledge regarding sodium intake and its role in hypertension and whether patients had undertaken lifestyle changes to reduce intake.
Principal Findings and Quantitative/Qualitative Results
Our data showed intervention clinics had a small but statistically significant decrease in both systolic and diastolic blood pressure (1.79mmHg p < 0.05; 1.31mmHg p < 0.01) between December 2012 and March 2013. Control clinics had no statistical difference in either systolic or diastolic blood pressure (0.132mmHg p=0.779; 0.706mmHg p =0.09) over the same time period. Additionally, data compiled using the questionnaires yielded encouraging results. Although not statistically significant survey responses indicated patients from intervention clinics were more likely to report increased knowledge of salt intake guidelines and implementation of healthier lifestyle changes related to reduced sodium intake.
Conclusions/Impact on Health Centers
Our research concluded that there was a statistically significant decrease in both systolic and diastolic blood pressure measurements among patients receiving care at intervention clinics. Our study results indicate that the use of informational posters and handouts may be an inexpensive and effective method that complements the current standard of care for blood pressure control among adult patients. Though not statistically significant, patients at intervention clinics were more likely to report improved knowledge and better dietary practices regarding daily sodium intake. Therefore similar interventions may be an effective approach for combating the increasing prevalence of hypertension among community health centers.
Limitations of the Study
uring the duration of the research study, a few limitations arose that are deserving of further consideration. First, data was collected over a short period of time. We feel it is therefore possible that had data been collected over a longer period of time a more clinically significant decrease in blood pressure measurements may have been observed. Second, our study excluded the pediatric population largely due to differences in the underlying pathophysiology of hypertension. Therefore, it remains unclear whether our study would have any effect among this particular patient population. Further research is needed. Lastly, we limited our posters and handouts on sodium reduction strategies to English and Spanish only, effectively eliminating all other patients who either do not speak these languages or have low language competencies.