Pre-planning Visit Quality Tool and immunization rates
in the Lutheran Family Health Center network
The way healthcare is delivered in this country is rapidly changing because of increased demands for services, the economics of providing affordable healthcare, and the need to ensure quality healthcare.
As part of ATSU’s mission for service, SOMA has included community healthcare as a significant part of its progressive medical school curriculum. Students spend the first year learning on campus, then the next three years providing affordable osteopathic healthcare to patients in community clinics in traditionally underserved neighborhoods.
In this way, even before beginning their medical career as a Doctor of Osteopathic Medicine, students can begin making a difference in improving whole healthcare for individuals in need during their early medical training. The patients benefit from the high quality of care provided by SOMA students – at rates affordable to them.
Research Objectives
The project will measure baseline immunization rates among 11-month-old to 12-month-old infants in the Lutheran Family Health Center network (LFHCN). The Pre-Planning Visit (PPV) tool will be implemented and immunization rates will be measured post-implementation. The Impact of race and primary language on immunization rates will also be considered.
Study Design and Methods
The PPV tool provides information about a patient’s immunization status, required vaccines and demographics. Baseline immunization rates among 11-month-old to 12-month-old infants within LFHCN were recorded using the PPV tool, and phone calls were made to all patients with verified delinquent statuses. Parents and/or guardians were notified of their child’s immunization status and were encouraged to make appointments with their provider. Six weeks post-phone call, data was compared to the latest immunization status to determine if the use of the PPV tool, in combination with telephone calls resulted in an increased rate of immunizations among 11-month-old to 12-month-old infants.
Principal Findings and Results
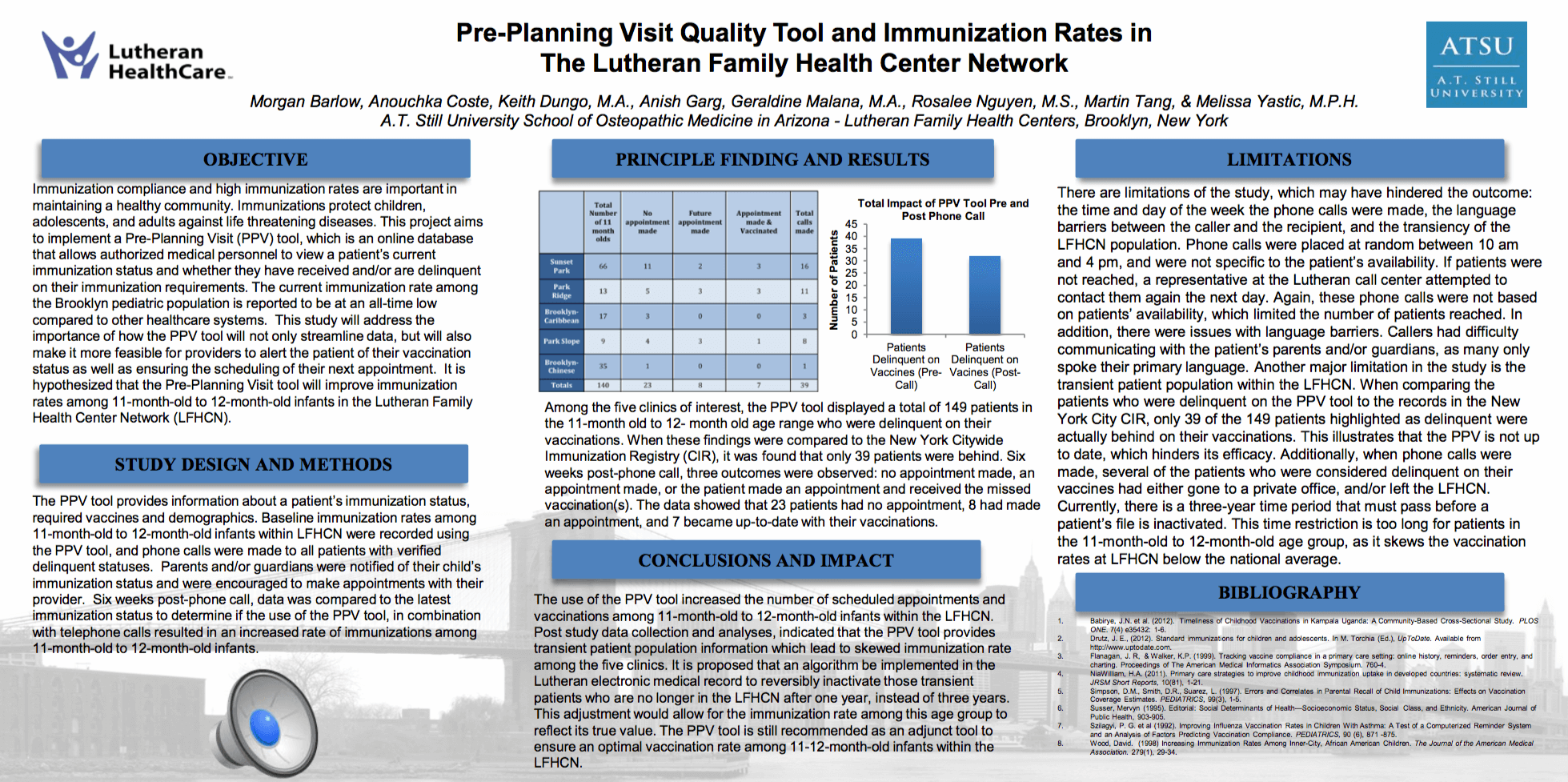
Among the five clinics of interest, the PPV tool displayed a total of 149 patients in the 11-month old to 12- month old age range who were delinquent on their vaccinations. When these findings were compared to the New York Citywide Immunization Registry (CIR), it was found that only 39 patients were behind. Six weeks post-phone call, three outcomes were observed: no appointment made, an appointment made, or the patient made an appointment and received the missed vaccination(s). The data showed that 23 patients had no appointment, 8 had made an appointment, and 7 became up-to-date with their vaccinations.
Conclusions and Impact on Health Centers
The use of the PPV tool increased the number of scheduled appointments and the number vaccinated among 11-month-old to 12-month-old infants within the LFHCN. However, the tool highlights that there is a transient patient population within the database, skewing the true immunization rate. It is proposed that a new algorithm be implemented in the Lutheran electronic medical record system. This addition would reversibly inactivate those transient patients who are no longer in the LFHCN after one year instead of three. This adjustment would allow for the immunization rates among this age group to reflect its true value.
LIMITATIONS
There are limitations of the study, which may have hindered the outcome: the time and day of the week the phone calls were made, the language barriers between the caller and the recipient, and the transiency of the LFHCN population. The phones calls were made on a Monday—an arbitrary day to start the study. It was decided to start the study on a Monday and end on a Friday in order to allow six full business-weeks to conduct the research. The time of day the individual phone calls were placed resulted in limitations, as the PPV tool did not provide the preferred time to contact patients. Phone calls were placed at random between 10 am and 4 pm, and were not specific to the patient’s availability. If patients were not reached, a representative at the Lutheran call center attempted to contact them again the next day. Again, these phone calls were not based on patients’ availability, which limited the number of patients reached.
In addition, there were issues with language barriers. Callers had difficulty communicating with the patient’s parents and/or guardians, as many only speak Spanish. The PPV tool indicates the preferred language, however this was not taken into consideration prior to the execution of this study. Another major limitation in the study is the transient patient population within the LFHCN. When comparing the patients who were delinquent on the PPV tool to the records in the New York City CIR, only 39 of the 149 patients highlighted as delinquent were actually behind on their vaccinations. This illustrates that the PPV is not up to date, which hinders its efficacy. Additionally, when phone calls were made, several of the patients who were considered delinquent on their vaccines had either gone to a private office, and/or left the LFHCN. Currently, there is a three-year time period that must pass before a patient’s file is inactivated. This time restriction is too long for patients in the 11-month-old to 12-month-old age group, as it skews the vaccination rates at LFHCN below the national average.