Triggering Adverse Events of Dentistry in a Rural Community Health Center
Contributors:
Parker Crutchfield
Hajera Azam
Dhwani Joshi
Valerie Paulo
Brooke Sabia
Jacksie Short
Parker Crutchfield
Hajera Azam
Dhwani Joshi
Valerie Paulo
Brooke Sabia
Jacksie Short
Participating Organizations:
A.T. Still University
A.T. Still University
Objectives
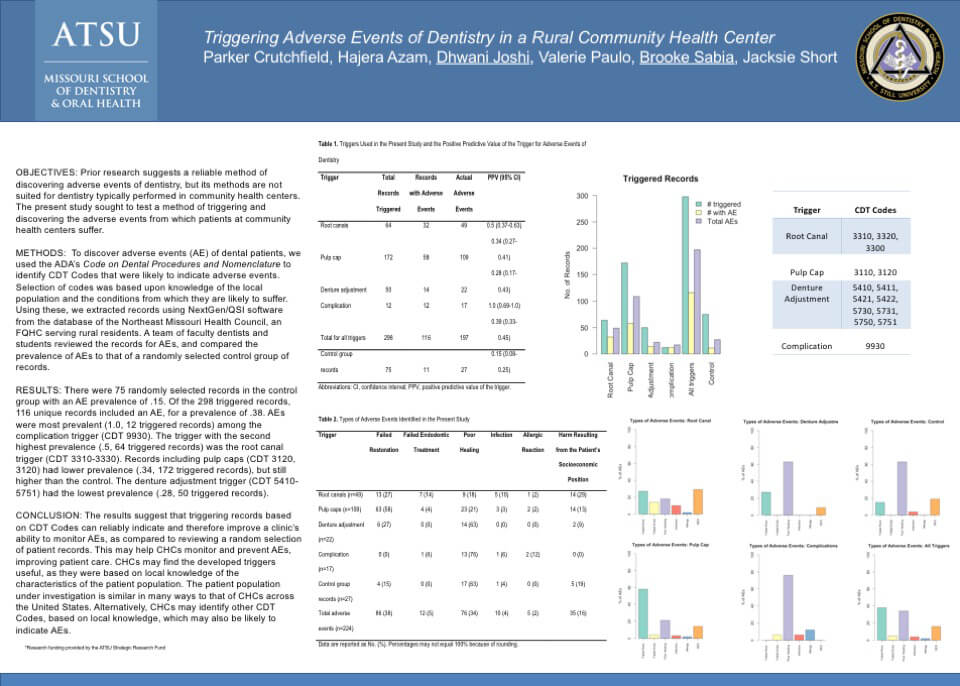
Prior research suggests a reliable method of discovering adverse events of dentistry, but its methods are not suited for dentistry typically performed in community health centers. The present study sought to test a method of triggering and discovering the adverse events from which patients at community health centers suffer.
Prior research suggests a reliable method of discovering adverse events of dentistry, but its methods are not suited for dentistry typically performed in community health centers. The present study sought to test a method of triggering and discovering the adverse events from which patients at community health centers suffer.
Methods
To discover adverse events (AE) of dental patients, we used the ADA’s Code on Dental Procedures and Nomenclature to identify CDT Codes that were likely to indicate adverse events. Selection of codes was based upon knowledge of the local population and the conditions from which they are likely to suffer. Using these, we extracted records using NextGen/QSI software from the database of the Northeast Missouri Health Council, an FQHC serving rural residents. A team of faculty dentists and students reviewed the records for AEs, and compared the prevalence of AEs to that of a randomly selected control group of records.
To discover adverse events (AE) of dental patients, we used the ADA’s Code on Dental Procedures and Nomenclature to identify CDT Codes that were likely to indicate adverse events. Selection of codes was based upon knowledge of the local population and the conditions from which they are likely to suffer. Using these, we extracted records using NextGen/QSI software from the database of the Northeast Missouri Health Council, an FQHC serving rural residents. A team of faculty dentists and students reviewed the records for AEs, and compared the prevalence of AEs to that of a randomly selected control group of records.
Results
There were 75 randomly selected records in the control group with an AE prevalence of .15. Of the 298 triggered records, 116 unique records included an AE, for a prevalence of .38. AEs were most prevalent (1.0, 12 triggered records) among the complication trigger (CDT 9930). The trigger with the second highest prevalence (.5, 64 triggered records) was the root canal trigger (CDT 3310-3330). Records including pulp caps (CDT 3120, 3120) had lower prevalence (.34, 172 triggered records), but still higher than the control. The denture adjustment trigger (CDT 5410-5751) had the lowest prevalence (.28, 50 triggered records).
There were 75 randomly selected records in the control group with an AE prevalence of .15. Of the 298 triggered records, 116 unique records included an AE, for a prevalence of .38. AEs were most prevalent (1.0, 12 triggered records) among the complication trigger (CDT 9930). The trigger with the second highest prevalence (.5, 64 triggered records) was the root canal trigger (CDT 3310-3330). Records including pulp caps (CDT 3120, 3120) had lower prevalence (.34, 172 triggered records), but still higher than the control. The denture adjustment trigger (CDT 5410-5751) had the lowest prevalence (.28, 50 triggered records).
Conclusion
The results suggest that triggering records based on CDT Codes can reliably indicate and therefore improve a clinic’s ability to monitor AEs, as compared to reviewing a random selection of patient records. This may help CHCs monitor and prevent AEs, improving patient care. CHCs may find the developed triggers useful, as they were based on local knowledge of the characteristics of the patient population. The patient population under investigation is similar in many ways to that of CHCs across the United States. Alternatively, CHCs may identify other CDT Codes, based on local knowledge, which may also be likely to indicate AEs.
The results suggest that triggering records based on CDT Codes can reliably indicate and therefore improve a clinic’s ability to monitor AEs, as compared to reviewing a random selection of patient records. This may help CHCs monitor and prevent AEs, improving patient care. CHCs may find the developed triggers useful, as they were based on local knowledge of the characteristics of the patient population. The patient population under investigation is similar in many ways to that of CHCs across the United States. Alternatively, CHCs may identify other CDT Codes, based on local knowledge, which may also be likely to indicate AEs.