General Goal: To know the major cause of these clinical syndromes and how they are transmitted.
Specific Educational Objectives: The student should be able to:
1. describe the differences between the various syndromes. Know the most common causes of the various clinical syndromes and what persons are more likely to get these infections.
2. describe any peculiar signs or symptoms and identify etiological agent that causes them (bulging fissure, currant jelly sputum, pneumatoceles).
Reading: Mosby's Color Atlas and Text of Infectious Diseases by Christopher P. Conlon and David R. Snydman. pp. 67-76.Lecture: Dr. Neal R. Chamberlain
References:
The following syndromes we will discuss are as follows:
The signs and symptoms of this particular syndrome are also seen in other syndromes (some infections of the immunocompromised host, and in the aspiration-prone patient, pneumonias of the newborn and infant). This is because the other syndromes also include bacteria that elicit respiratory symptoms, sudden onset, and purulent sputum. However, the circumstances and immune status of the patient tend to increase the chances of acquiring a different set of bacterial pathogens.
1. Etiology and epidemiology
Community Acquired
Streptococcus pneumoniae is a bacterial pathogen that affects children and adults worldwide. It is a leading cause of illness in young children and causes illness and death among the elderly and persons who have certain underlying medical conditions. Pneumococcal infection causes an estimated 40,000 deaths annually in the United States. Approximately half of these deaths potentially could be prevented through the use of vaccine. Despite appropriate antimicrobial therapy and intensive medical care, the overall case-fatality rate for pneumococcal bacteremia is 15%-20% among adults. The organism colonizes the upper respiratory tract and can cause the following types of illnesses: a) disseminated invasive infections, including bacteremia and meningitis; b) pneumonia and other lower respiratory tract infections; and c) upper respiratory tract infections, including otitis media and sinusitis. Each year in the United States, pneumococcal disease accounts for an estimated 3,000 cases of meningitis, 50,000 cases of bacteremia, 500,000 cases of pneumonia, and 7 million cases of otitis media.
In adults, 60%-87% of pneumococcal bacteremia is associated with pneumonia. Severe pneumococcal infections result from dissemination of bacteria to the bloodstream and the central nervous system. In the United States, the risk for acquiring bacteremia is lower among white persons than among persons in other racial/ethnic groups (i.e., blacks, Alaskan Natives, and American Indians). Black adults have a threefold to fivefold higher overall incidence of bacteremia (49-58 cases per 100,000 population) than whites (5-8). Rates of invasive pneumococcal disease are exceptionally high among Alaskan Natives and American Indians. At least 500,000 cases of pneumococcal pneumonia are estimated to occur annually in the United States; S. pneumoniae accounts for approximately 25%-35% of cases of community-acquired bacterial pneumonia in persons who require hospitalization. Concomitant bacteremia occurs in approximately 10%-25% of adult patients who have pneumococcal pneumonia
H. influenzae and K. pneumoniae are more commonly seen in patients with COPD, alcoholics, and the elderly.
S. aureus infections are most common in IV drug users, the elderly, in people with a recent influenza virus infection, and in individuals with cystic fibrosis.
P. aeruginosa is also often seen as a cause of pneumonia in patients with cystic fibrosis and those with severely compromised respiratory defenses. Patients on respirators are more likely to develop pneumonia due to P. aeruginosa.
S. pyogenes pneumonia is less common today due to the use of antibiotics to treat upper respiratory tract infections.
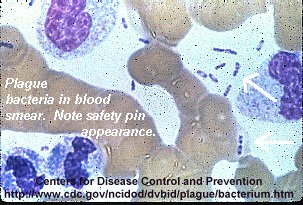
N. meningitidis is occasionally seen in epidemics in military recruits. Y. pestis infections are due to environmental exposure to an infected rat population. B. pseudomallei infections are due to exposure with contaminated soil in Southeast Asia.
2. Clinical, Radiologic, and Laboratory Features
Pulmonary symptoms include any combination of symptoms listed below:
Exceptions: patients who are severely dehydrated, patients with obstructive lesions, and patients too weak to mount an effective cough. The odor of the sputum should be noted since anaerobic bacterial infections often times produces a foul smelling sputum.
Microscopic examination of the sputum should reveal numerous PMNs, occasional alveolar macrophages, and many bacteria. Large numbers of squamous epithelial cells suggests contamination with saliva and as a result cannot be used for diagnostic evaluation.
Other samples that should be taken include a blood sample used to culture for bacteria and culture of pleural effusions if present. White blood counts of the blood sample reveal a leukocytosis with a predominance of early forms of PMNs (bands).
3. Diagnosis
Differential Features of Common Bacterial Pathogens:
| Bacterial Pathogens | Susceptibility | Clinical Features | Associated Sites of Infection | Sputum Gram Stain |
| S pneumoniae | Children< 2, adults over 65, Splenectomy, Chronic lymphatic leukemia, Multiple myeloma, Sickle cell anemia, Postinfluenza, COPD, smokers | Rusty sputum Single shaking chill | Bacteremia 25-50% Pleural effusions Arthritis Meningitis Endocarditis Sinusitis | Encapsulated lancet-shaped Gram-positive diplococci or short chains Quellung reaction positive |
| H. influenzae | Young children < 2, COPD, Alcohol abusers, Postinfluenza | Pleural effusion common Bacteremia | Otitis Sinusitis Meningitis Epiglottis Facial infection | Small Gram-negative pleomorphic encapsulated bacillus (Group B) Occasionally disease caused by nontypable strains |
| S. aureus | Metastatic infection in parenteral drug abusers or patients with infected intravenous catheters, Postinfluenza, Cystic fibrosis, In hospital aspiration | Pleuritic chest pain Multiple thin walled abscesses ("pneumatoceles") Cardiac murmurs | Endocarditis Cerebritis Metastatic abscesses Skin furuncles | Gram-positive cocci in clusters |
| S. pyogenes | Postinfluenza, COPD | Pleural effusion or empyema (up to 90%) Bacteremia 12% | Tonsillitis Mediastinitis | Gram-positive cocci in chains Quellung reaction negative |
| K pneumoniae | Alcohol abusers, COPD, Neonates Nosocomial | "Currant jelly" sputum Bulging fissure Lung necrosis | Large Gram-negative rod with capsule | |
| P. aeruginosa | Neutropenic, Intubated respiratory therapy, ICU-Burn unit, Cystic fibrosis | Green sputum Fulminant course Necrotizing with multiple small and large abscesses | Skin lesions (ecthyma gangrenosum) | Gram-negative rod (encapsulated in patients with cystic fibrosis) Enteric bacilli Same as P. aeruginosa Variable -- Gram-negative rod |
| Enteric bacilli | Same as P. aeruginosa | Variable -- Gram-negative rod |
B. Atypical Pneumonia Syndrome:
These infections can involve Mycoplasma, Chlamydia, Rickettsia,
other bacteria, viruses, or fungi. Determining the causative agent requires
knowing what the common causes of atypical pneumonia are, as well as knowing
the epidemiology, clinical picture, radiologic findings, and laboratory
findings. This will provide the presumptive diagnosis. The definitive diagnosis
usually requires retrospective serologic tests.
Comparative Epidemiologic Features of the Atypical Pneumonias:
| Atypical pneumonias | Incubation period (days) | Seasonality | Patient Age | Exposure to Infected Animal or Sources | Person to person Transmissions | Underlying Chronic Diseases |
| Mycoplasma pneumonia | 14-21 | Year round | Adolescents and young adults | - | + | - |
| Legionnaire's disease | 2-10 | Year round (summer peak) | Adult | Cooling towers, condensers, excavation sites | - | + |
| Psittacosis | 7-14 | Year round | Adult | Psittacine birds, pigeons, turkeys, pet shops, zoos | - | - |
| Q fever | 14-28 | Year round | Adult | Cattle, sheep, goats, contaminated milk, birthing various livestock | - | - |
| Tularemia | 1-14 | Year round | Adult | Rabbits, ticks | - | - |
| Anthrax | 1-5 | Year round | Adult | Goat hair/skin, wool, bonemeal fertilizer | - | - |
| Viral pneumonia | 1-3 | Winter | All | + | + | |
| Histoplasmosis | 3-21 | Year round | All | Chickens, bats, river valleys | - | - |
| Coccidioidomycosis | 7-28 | Year round | All | California, Southwest USA | - | - |
Symptoms of atypical pneumonia include fever, nonproductive cough, and prominent constitutional signs (severe headache, malaise, myalgias) onset is usually more insidious. Physical examinations at most disclose rales and rhonchi. Signs of pulmonary consolidation are rarely present. The radiographic findings usually appear as interstitial patchy bronchopneumonic infiltrates.
There is a lot of overlap in the manifestations of atypical pneumonia however the following table indicates some distinctive features that can aid in differentiation.
| Atypical Pneumonias | Clinical Features | Radiographic Features | Laboratory Features |
| Mycoplasma pneumonia | Upper respiratory tract symptoms, Bullous myringitis, Hemolytic anemia, Myocarditis, Meningoencephalitis | Occasional pleural effusion | Cold hemagglutinins |
| Legionnaire's disease | Relative bradycardia, Abdominal pain, Vomiting and diarrhea, Hematuria, Mental confusion | Occasional pleural effusion | Abnormal liver and renal function tests Increased CPK |
| Psittacosis | Relative bradycardia Epistaxis Horder's spots Splenomegaly | -- | Normal or low leukocyte count |
| Q fever | Relative bradycardia, Tender hepatomegaly, Endocarditis | -- | Abnormal liver function tests |
| Tularemia | Substernal chest pain, Relative bradycardiaBilateral hilar adenopathy common | Bilateral hilar adenopathy common, Occasional bloody pleural effusion | Normal or low leukocyte count |
| Anthrax | Precordial discomfort, Hemorrhagic meningitis | Mediastinal adenopathy common, Occasional pleural effusion | -- |
| Viral pneumonia | Upper respiratory tract symptoms | -- | -- |
| Histoplasmosis | Erythema nodosum, Substernal discomfort | Bilateral hilar adenopathy common | tuberculate macroconidia in vitro)
yeast form in tissue |
| Coccidioidomycosis | Chest pain, Erythema nodosum | Bilateral hilar adenopathy common, Occasional pleural effusion | Arthroconidia in vitro
Spherule in tissue |
Direct isolation of the organism is not usually performed due to the hazardous nature of some organisms (F. tularensis) and due to the specialized culture techniques needed to allow growth of the organism. Microscopic examination of the sputum is not performed unless a Legionella sp. infection is suspected. This organism is stained with Dieterle silver stain and direct fluorescent antibody staining. A test for Legionella antigen in the urine is available and can be useful. Legionella can now be routinely cultured and this may also aid the physician in determining a definitive diagnosis. An indirect Fluorescent Antibody test to detect antibodies to Mycoplasma pneumoniae is very useful.
Serologies for the various causes of atypical pneumonia include:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}