{kind=link}
{kind=link}
{kind=link}
|
|
 |
General Goal: To know the major cause of these clinical syndromes and how they are transmitted.
Specific Educational Objectives: The student should be able to:
1. describe the differences between the various syndromes. Know the most common causes of the various clinical syndromes.
2. accurately describe how to perform a mantoux test and interpret the results.
3. describe any peculiar signs or symptoms and identify etiological agent that causes them. Know the fungal forms of the dimorphic fungi that can be found in the lung.
Reading: Mosby's Color Atlas and Text of Infectious Diseases by Christopher P. Conlon and David R. Snydman. pp. 67-76.Lecture: Dr. Neal R. Chamberlain
References:
A. Typical
Pneumonia Syndrome
B. Atypical
Pneumonia Syndrome
C. Chronic Pneumonias
D. Pneumonias of the Newborn
Period and Infancy
E. Pneumonia in the
Aspiration-Prone Patient
F. Pulmonary
Infection in the Immunocompromised Host
These pneumonias develop gradually over a period of weeks to months and are caused by numerous microorganisms. Noninfectious as well as infectious processes can result in chronic pneumonia however, we will only be concerned with the infectious causes of chronic pneumonia.
Dark-skinned people and pregnant women show an increased tendency to develop disseminated or chronic pulmonary forms of Coccidioides immitis. White-skinned males are more likely to develop chronic cavitary histoplasmosis. Nocardiosis, cryptococcoses and mycobacterial disease are associated with hosts with defects in cell-mediated immunity. Opportunistic fungal infections are also more common in immunocompromised patients (histoplasmosis, blastomycosis, coccidioidomycosis).
1. Clinical, Radiologic, and Laboratory Features
Often times the patient experiences low grade fever, anorexia, significant weight loss, a productive cough, hemoptysis, chest pain and dyspnea (onset very gradual). A putrid odor of the sputum is a sure indication of an anaerobic infection.
Also, certain microorganisms can infect extrapulmonary sites which helps to narrow down the number of possible causative agents.
| Disease | Location | Source/ Mode
of Spread |
Predisposing Underlying Conditions | Extrapulmonary manifestations | Characteristic Chest X-ray |
| Actinomycosis | Worldwide | Normal oral flora/Aspiration | None | Rib destruction Cutaneous sinuses | Mass lesion or dense infiltrate, cavitation, spread to pleura and chest wall |
| Nocardiosis | Worldwide | Soil decaying vegetable
matter/ Inhalation |
Defect cell-mediated immunity;
High dose corticoste- roid therapy; Alveolar proteinosis Chronic granulo- matous disease of childhood |
Brain abscess Skin and subcutaneous abscess | Confluent broncho-
pneumonia; Cavitation Pleural and chest wall involvement |
| Melioidosis
B. pseudomallei |
Between 20° N and 20° S latitudes in S.E. Asia | Soil, stagnant water/Inhalation | None | Skin and subcutaneous
abscess |
Lymphadenitis, Nodular infiltrates in upper lobes Cavitation |
| Mixed anaerobic pleuropulmonary disease | Worldwide | Normal oral flora/Aspiration | Alcoholism Neurologic disease Esophageal disorder Seizure disorder
Recent
general anesthesia |
Brain abscess | Dependent
lung segments, single or multiple cavities with surrounding infiltrate; frequent air fluid level; frequent pleural involvement |
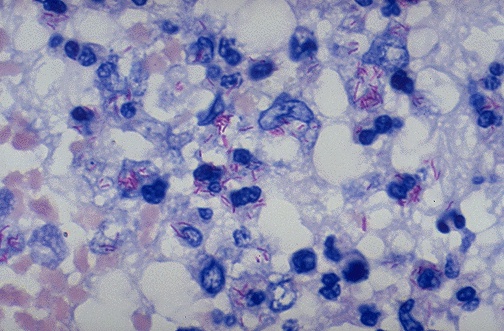
| Tuberculosis | Worldwide | Person-to-person | Alcoholism Silicosis Gastrectomy Defective cell-mediated immunity Diabetes mellitus Corticoste- roid therapy | Meningitis, osteomyelitis Lymphadenitis Infiltration of liver
and bone marrow Pericarditis Genitourinary involvement Addison's disease |
Multiple thick-walled cavities with surrounding infiltrate in upper lobe, often bilateral |
| M. kansasii | Worldwide, but especially Texas, Louisiana, Chicago | Unknown | Chronic obstructive pulmonary disease (COPD) Silicosis | Indistinguish- able from tuberculosis; pleural involvement rare | |
| M. avium-
intracellulare |
S.E. United States | Soil | COPD Silicosis Defective cell-mediated immunity | Rare except in immuno- compromised hosts | See above |
| North American blastomycosis
broad-based budding yeast in tissue |
S.E. and Mid-Atlantic United States; Great Lakes region; Manitoba; Africa | Soil, Domestic animals | None | Skin, bone and genito-urinary tract | Fibronodular, interstitial or alveolar infiltrates, often segmental or lobar |
| Coccidioidomycosis
Arthroconidia in vitro Spherule in tissue |
S.W. United States; parts Central America | Soil | Greater tendency to disseminate in dark-skinned people or pregnant females | Skin, bone or meninges | Thin-walled, solitary cavities, segmental, alveolar infiltrate with hilar adenopathy |
| Histoplasmosis
tuberculate macroconidia in vitro yeast form in tissue |
Ohio and Mississippi valleys; endemic foci in 31 states | Soil contaminated with large amount of bird or bat excreta | Extremes of life for disseminated disease; emphysema for chronic cavitary histoplasmosis | Oral mucosal ulcerations, hepato- splenomegaly; infiltration of bone marrow, Addison's disease, mediastinitis | Thick-walled, expanding cavities, interstitial or pathy, nodular infiltrates with hilar adenopathy |
| Disease | Location | Source/ Mode of Spread | Predisposing Underlying Conditions | Extrapulmonary Manifestations | Characteristic Chest X-ray |
| Crypto- coccosis | Worldwide | Soil contam- inated with bird droppings | Defects in
cell-mediated immunity; corticosteroid therapy; lympho- proliferative disorders; alcoholism, diabetes mellitus |
Meninges, skin, occasionally bone | Nodular dense infiltrates in
lower lobes; cavitation rare |
| South
American blasto- mycosis |
South and Central America | Soil | None | Skin, oral
mucosa, lymph nodes |
Bilateral
alveolar infiltrates in lower lobes; often interstitial infiltrates broad-base budding yeast
|
| Sporo- trichosis | Worldwide | Vegetable matter | None | Upper lobe, thin-walled cavities,
unilateral |
|
| Paragon- imiasis | Far East Asia; India; Africa; Central and South America | Consumption of raw or pickled fresh water crustacea | None | Rarely abdominal
or central nervous system involvement |
Cavity often
with patchy infiltrates, pleural effusion |
| Echino- coccosis | Greece; Lebanon and other sheep and cattle-raising areas | Ingestion of material contaminated with dog feces | None | Hepatic cysts | Rounded,
nodular lesions |
| Amebiasis | Worldwide, primarily under-developed countries | Fecal-oral contamination | Male homosexuals | Intestinal amebiasis Hepatic abscess | Infiltrative or cavitary lesion
in right lower lobe, often with right pleural effusion |
2. Diagnosis
These are five basic modalities that can aid in diagnosis:
Culture of the sputum depends on the sample. Anaerobes like Actinomyces require translaryngeal aspiration and culture in the absence of oxygen. Some of the organisms like Nocardia require 3 to 4 days to grow even though they are aerobes and since sputum cultures are routinely discarded at 48 hours you need to inform the lab that you suspect a nocardiosis. Mycobacterial cultures also require special treatments and placement on special media therefore informing the lab of such infections is essential.
Culture of fungi will vary with the organism. Generally, cryptococcoses is hard to obtain from the lung (only about 50% recovery). Coccidioidomycosis, blastomycosis, and sporotrichosis are usually quite easy to culture (about 70-100% recovery). Culturing of pleural fluid, skin, urine, prostate secretions, may provide material that will yield a positive culture and definitive diagnosis.
Skin testing is of limited value for determining a fungal etiology, however, it is very useful in the diagnosis of tuberculosis. Conversion from a recent negative skin test to a positive test is a strong indication of tuberculosis in adults. The Mantoux test requires 48-72 hours before it is read. The zone of induration is read not the zone of erythema. Click here for proper way to inject and measure the results of the Mantoux test.. Whether a reaction to the Mantoux tuberculin skin test is classified as positive depends on the size of the induration and on the person's risk factors for TB.
An induration of 5 or more millimeters is considered a positive reaction for the following people:
Serology can be very useful in assisting you in diagnosis. There are serologic tests for Nocardia and for melioidosis. Serology is very useful in diagnosis of fungal and parasitic infections. Complement fixation, hemagglutination, and immunodiffusion tests are available to assist in diagnosis of fungal and parasitic chronic pneumonias.
When all else fails invasive methods to obtain samples directly from the lungs can be obtained. These methods include translaryngeal aspiration, open lung biopsy, needle biopsy of the lung, and transbronchial biopsy via fiberoptic bronchoscopy.
3. Treatment
Due to the large diversity of organisms in this group antibiotic treatment should not be instituted until your sure of the cause of the infection.
D. Pneumonias of the Newborn Period and Infancy:
1. Etiology and Epidemiology
The causes of pneumonia occurring in pediatric patients vary according to the age of the patient.
day 0 to 2 weeks
Respiratory distress is the most frequent indication for placing the neonate in an intensive care nursery. LRT infections account for the major portion of pulmonary disease during the first 28 days of life and are an important cause of neonatal mortality and morbidity.
Infectious pneumonias in neonates can be placed in three different categories based on time of acquisition and age presentation.
2. Infections acquired during labor and delivery. This is the most commonly seen. The organisms are transmitted to the infant by upward spread of bacteria from the maternal genital tract into the amniotic cavity. The fetus aspirates or inhales the infected amniotic fluid prior to birth. Mostly, you see infections with pathogens colonizing the female genital tract. Usually, Group B Streptococcus (S. agalactiae), E. coli, and Klebsiella pneumoniae are the cause of pneumonia in these infants.
3. Infections acquired after birth. These pneumonias present at various times after birth. The organisms can include RSV, parainfluenza, influenza virus, echoviruses, coxsackie viruses, adenoviruses, Chlamydia trachomatis, Staphylococcus aureus, and Gram-negative enteric bacteria. The virus infections are usually acquired in late fall to early spring.
Many different agents can cause pneumonia in these patients. As a result the clinical, radiologic, and laboratory features are highly variable.
In viral and Chlamydial pneumonic infections the patient experiences apnea, tachypnea, lethargy, and respiratory distress. Little to no sputum is produced. X-rays reveal diffuse, interstitial or patchy infiltrates. Rarely one sees consolidation. In all but Chlamydial pneumonia a fever (103-104° F) is present. The bacterial infections usually are like that presented for people with typical pneumonia syndrome. Please note, clinical, radiologic, and laboratory features in preterm neonates are quite different but will not be covered in this course.
3. Diagnosis
The etiologic agent most likely to cause infection depends on the age of the patient, if the mother acquired a TORCH infection during pregnancy, if the mother's vagina was colonized with a particular organism, the clinical and radiologic features, as well as the presence of infection in other body sites.
4. Prevention
Screen mother's blood for rubella titers. Also screen her blood for
syphilis. A good history may indicate if the mother has had genital herpes.
If she has then preparations for a C-section at delivery may be necessary.
Obtain vaginal/rectal swab samples at 35 to 37 weeks' gestation and culture
for Streptococcus agalactiae (leading cause of neonatal sepsis).
If positive for Group B strep then treat the mother while still pregnant
with antibiotics to eliminate the organism. This will lower Group B strep
infections by about 78%.
E. Pneumonia in the Aspiration-Prone Patient
Aspiration is a process in which matter present in the oropharynx is carried through inhalation into the lower tracheobronchial tree. Usually the matter is cleared from the lungs however, if the person is compromised in some fashion or inhales large amounts of matter a pneumonia can result.
Aspiration includes several aspiration syndromes.
2. Reflex Airway Closure: Aspiration of inert fluids (water, saline, nasogastric feedings) may produce laryngospasm and pulmonary edema with resultant hypoxemia. Treatment includes intermittent positive-pressure breathing with 100% O2 and isoproterenol.
3. Mechanical Obstruction: Aspiration of inert fluid or particulate matter (partially digested food, hot dogs, peanuts) may produce simple mechanical obstruction. Coughing, wheezing, and dyspnea occur with atelectasis seen on X-ray of the chest. Treatment requires tracheobronchial suction and removal of the particulate matter by fiberoptic bronchoscopy.
4. Aspiration Pneumonia: Aspiration of bacteria from the oropharynx. Patients have a cough, fever, purulent sputum, and radiographic evidence of infiltrate. Treatment requires antibiotics. This is what we will discuss in this class.
The following conditions predispose patients to aspiration pneumonia.
| COMMUNITY ACQUIRED | HOSPITAL ACQUIRED |
Obligate anaerobes
|
Obligate anaerobes
|
Facultative aerobes
|
Facultative aerobes
|
2. Clinical, Radiographic, and Laboratory Features
Aspiration pneumonia is much like "typical" pneumonia. However, the possibility of necrotizing pneumonia and lung abscess are more likely in aspiration pneumonia. Often times the sputum has a very foul odor that is pathognomonic for anaerobic lung infections.
3. Diagnosis
This syndrome is a lot like "Typical" pneumonia except for recurrent chills, pneumonia in dependent lung segments, and growth of normal flora on routine sputum culture. Some patients (50%) will produce foul smelling sputum. To get a definitive diagnosis translaryngeal aspiration must be performed. However, this is a dangerous procedure and usually the patients are treated empirically on the basis of predicted bacteriology.
F. Pulmonary Infections of the Immunocompromised Patient
These patients are often troubled with respiratory infections which due to their poor immunologic response to invaders are in serious trouble. Unfortunately, many different organisms can cause respiratory disease in these patients. The patients prognosis is often linked to whether they have neutropenia. Patients with neutropenia are often quite rapidly killed by pneumonic infections and require aggressive diagnostic methods (open lung biopsy) and treatments.
Combination antimicrobial therapy is often used to cover the large number of possible organisms causing disease.
1. Epidemiology and Etiology
Most pulmonary infections of the immunocompromised patient are bacterial. The following organisms can cause infections:
Bacteria (most common to least common)
2. Diagnosis
- Aspergillus sp.
- Mucor sp.
- Candida albicans
A very good history and physical exam will help a lot. Knowledge of the most common organism causing pneumonia in a particular circumstance is also important. Acute onset of symptoms usually indicate a bacterial or Aspergillus infection. Subacute onset of symptoms indicate a viral, Pneumocystis, or Nocardial infection. A chronic onset of symptoms suggest infection due to mycobacteria, Nocardia, or fungi. Usually sputum is not produced in sufficient amounts to aid in diagnosis. Blood cultures can be useful and should be obtained. Skin tests are often useless because the person is unable to mount a T cell response. If samples prove useless and the patient is rapidly deteriorating even during empiric antimicrobial treatment then translaryngeal aspirates, open lung biopsy, or percutaneous needle biopsy are necessary to determine the exact etiologic agent.
Note: AIDS patients have a lot of problems with pneumonia and are
usually infected with Pneumocystis jiroveciior
Mycobacteria.
|
|
|
|