Severe Adult Respiratory Syndrome CoronaVirus-2 (SARS CoV-2)
COronaVIrus Disease 2019 (COVID 2019)
Neal R. Chamberlain, Ph.D., Department of Microbiology/Immunology, ATSU/Kirksville College of Osteopathic Medicine
Overview
SARS CoV-2 (old name 2019-nCoV) is the viral cause of COronaVIrus Disease 2019 or COVID-19. In December of 2019, SARS CoV-2 was identified as the cause of an outbreak of acute respiratory illness in Wuhan, China. As of March 19, 2020, there have been 229,336 cases of COVID-19 reported worldwide with over 10,000 cases reported in the US.
Etiology
SAR CoV-2 is a coronavirus (a positive sense single stranded RNA virus) named because of the crown-like appearance of the glycoprotein projections on the outer surface of the virus (see image below). Several variants of this virus have appeared (e.g., alpha, delta, omicron). Some are more infectious but less virulent (delta, omicron) than earlier variants (alpha). There are hundreds of coronaviruses. Most infect animals (pigs, camels, bats and cats). Occasionally, these animal coronaviruses can infect and cause disease in humans. This is called a spillover event.
https://phil.cdc.gov/Details.aspx?pid=18114
Seven different coronaviruses currently infect humans. Four cause the common cold (229E, OC43, NL63 and HKU1). Three coronaviruses can cause serious disease in humans; pneumonia, SARS (severe acute respiratory syndrome), sepsis, septic shock and multiorgan dysfunction.
The first of the serious coronaviruses, SAR CoV-1 emerged in late 2002 and disappeared by 2004. MERS CoV (Middle East Respiratory Syndrome) emerged in 2012 and remains in circulation in camels. The third coronavirus of the serious three is SAR CoV-2 and it emerged in December 2019 from China. Genome sequencing and phylogenic analysis indicated that SAR CoV-2 is a betacoronavirus in the same subgenus as SAR CoV-1 but in a different clade. SAR CoV-1 was a spillover event from bats to humans.
Many believe SAR CoV-2’s reservoir host was also from bats. However, differences between the bat coronavirus and SARS-CoV-2 suggest that an intermediate host infected humans. The intermediate host that infected humans with SARS-CoV-2 is unknown. Phylogenetic analysis of SARS-CoV-2 strains have identified two different types of SARS-CoV-2 so far. They are designated type L (70 percent of the strains) and type S (30 percent). The L type was most the most common cause of human infection during the early days of the epidemic in China. The S type accounts for most of the strains outside Wuhan, China. The clinical implications of these findings are currently unknown.
Manifestations
Incubation period- 14 days following exposure, with most manifesting infection about four to five days after exposure (median- 5.1 days).
Initial Presentation- The most common clinical features at the onset of illness are fever (99%), fatigue (70%), dry cough (59%), anorexia (40%), myalgias (35%), dyspnea (31%), and sputum production (27%) (Notice runny nose does not appear to be a common symptom. Rhinorrhea may indicate the patient has some other cause, other than SAR CoV-2, for their respiratory symptoms). NO clinical features can reliably distinguish COVID-19 from other viral respiratory infections.
Pneumonia appears to be the most frequent serious manifestation of infection. Symptoms include fever, cough, dyspnea, and bilateral infiltrates on chest imaging (ground glass opacities with or without consolidations in the periphery bilaterally on CT).
Presentations — Ranges from mild to critical. Most infections are not severe.
- Asymptomatic- percent is unknown
- Mild- fever, dry cough and dyspnea TO mild pneumonia - 81%
- Severe disease- dyspnea, hypoxia, or >50 percent lung involvement on imaging within 24 to 48 hours – 14%
- Critical disease- respiratory failure, shock, or multiorgan dysfunction – 5%
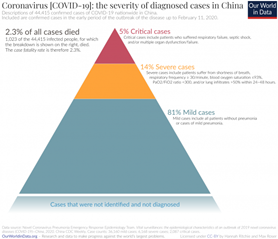
https://ourworldindata.org/coronavirus
Recovery- Appears to take around 2 weeks for mild infections and 3-6 weeks for severe disease.
Age and severity of illness — All ages of patients can acquire SARS-CoV-2. Adults of middle age and older are more likely to have symptoms of this infection. The median age for COVID-19 symptoms ranged from 49 to 56 years. In a report from China, 87 percent of patients were between 30 and 79 years old. A recent study in the US revealed that 38% of hospitalized patients with COVID-19 were between 20 and 54 years of age.
Symptomatic infection in children is uncommon. If symptoms occur in children, they are usually mild (low-grade fever, cough, sore throat, OR focal pneumonia on CT; no oxygen supplementation needed). Severe cases of COVID-19 have been reported in children. So far, all children with severe disease have recovered.
Between 2-6.3% of symptomatic infections were in individuals younger than 20 years old. Older age is also associated with a higher percent with symptoms and increased mortality (see graph below). The case fatality rate is around 8% for patients aged 70-79 and about 15% for patients 80 years or older.
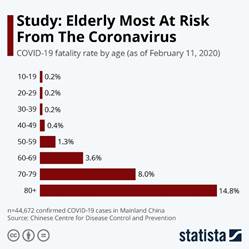
Other predisposing conditions for severe disease- Men have a higher fatality ratio than women. Patients with cardiovascular disease, diabetes, respiratory disease, hypertension and immunocompromised patients are more likely to manifest symptoms, develop severe disease and to die following infection with SARS CoV-2 (see graph below).

Complications- Some patients with mild symptoms progress over the course of a week to severe disease. In patients with pneumonia due to SARS CoV-2, dyspnea developed after 5-8 days following onset of symptoms Hospital admission occurred after a median of seven days of symptoms.
Acute respiratory distress syndrome (ARDS) is the most frequent complication in patients with severe disease. ARDS developed in 20 percent after about eight days, and mechanical ventilation was implemented in 12.3 percent. Age greater than 65 years, diabetes mellitus, and hypertension were each associated with ARDS.
Other less frequent complications include arrhythmias (17%), acute cardiac injury (7%) and shock (9%).
Overall case fatality rate is 1-3%. Fatality rate differs by country and age of the patient. No deaths were reported among noncritical cases.
Epidemiology
COVID-19 has spread, in four months’ time from China to 164 countries (March 20, 2020). The only continent with no reported cases is Antarctica. As of March 20, 2020, there have been 272,042 cases of COVID-19 reported worldwide with over 18,000 cases reported in the US. States in the US with the highest number of reported cases are New York, Washington, California, Florida, Massachusetts, New Jersey, Illinois and Colorado.
Updated case counts can be found on the World Health Organization and European Centre for Disease Prevention and Control websites.
Transmission — Understanding of the transmission risk is incomplete. Initially there was an association with people who worked or visited a seafood market in Wuhan, China that sold live animals. As the outbreak progressed, person-to-person spread became the main mode of transmission.
Person-to-person spread of SARS-CoV-2 occurs by respiratory droplets. Others have shown that the virus has a half-life survival rate of 1.3 h on these airborne droplets. Virus is released in the respiratory secretions when a person with infection coughs, sneezes, or talks to another person. If those droplets make contact with the mucous membranes (eye, nose, or mouth) a person can be infected. Droplets typically do not travel more than six feet and do not linger in the air; however, in one study, SARS-CoV-2 remained viable in aerosols under experimental conditions for at least three hours.
Infection can also occur if a person touches an infected surface and then touches their eyes, nose, or mouth. Preliminary research indicates that the virus is viable on plastic and stainless steel for up to three days, but does not survive on cardboard for more than 24 h or on copper for more than 4 h.
The reported rates of transmission from an individual with symptomatic infection vary by location and infection control interventions. According to a joint WHO-China report, the rate of secondary COVID-19 ranged from 1-5 percent in China. In the United States, the symptomatic secondary attack rate was 0.45%.
Viral RNA levels appear to be higher soon after symptom onset compared with later in the illness. Transmission might be more likely in the earlier stage of infection. The R nought (Ro) varies by study and has been calculated from 1.32 to 3.9.
Transmission of SARS-CoV-2 from asymptomatic individuals (or individuals within the incubation period) has also been described. However, the extent to which this occurs remains unknown.
SARS-CoV-2 RNA has been detected in blood and stool specimens. Live virus has been cultured from stool in some cases but fecal-oral transmission does not appear to be a significant factor in the spread of infection.
Pathogenesis
SARS-CoV-2 has four structural proteins, known as the S (spike), E (envelope), M (membrane), and N (nucleocapsid) proteins; the N protein holds the RNA genome, and the S, E, and M proteins together create the viral envelope. The spike protein allows the virus to attach to the membrane of a host cell.
Like SAR CoV-1, SAR CoV-2’s S-protein binds to the host cell receptor angiotensin converting enzyme 2 (ACE2). This host cell receptor is present on epithelial cells of the conducting airways (trachea, bronchi, bronchioles) and the alveoli (type 1 and 2 pneumatocytes).
After a SARS-CoV-2 virion attaches to a target cell, the host cell's transmembrane protease serine 2 (TMPRS2) cuts open the spike protein, exposing a fusion peptide. The virion’s RNA is then released into the cell. The host cell produces copies of the virus that can then infect more cells. SARS-CoV-2 produces several virulence factors that promote shedding of new virions and inhibit host immune response.
Destruction of the host epithelial cells causes an immunological response. This response brings in lymphocytes (T-cytotoxin cells; CD8 cells) to destroy the virus infected cells. A number of proinflammatory cytokines are also produced by the lymphocytes. One of the proinflammatory cytokines, interleukin-1 (IL-1), can cause the fever seen in many patients with this viral infection. The immune response increases the amount of interstitial fluid in the walls of the conducting airways and alveoli. On chest radiograph this can be seen as an infiltrate.
At the same time the immune response results in partial filling of the alveoli with fluid from the vasculature. This partial filling results in the ground glass appearance of the lungs on CT. If the immune response does not eliminate the infection at this stage then the virus can gain access to the blood stream and be transported systemically.
This viremia can cause even more proinflammatory cytokines to be produced. If high concentrations of these cytokines are produced it can result in a cytokine storm resulting in septic shock and multiorgan dysfunction.
Diagnosis
Clinical suspicion and testing criteria- Since there is no proven treatment or vaccine, initial management should focus on early recognition of suspect cases, immediate isolation and institution of infection control measures.
1. The possibility of COVID-19 infection should be considered in patients with fever and/or respiratory tract symptoms (e.g., cough, dyspnea) who have had any of the following in the prior 14 days:
- Close contact with a confirmed/suspected COVID-19 infected person. This includes work in health care settings. Close contact means being within six feet of a patient for a prolonged period while not wearing personal protective equipment (PPE) or having direct contact with infectious secretions while not wearing PPE.
- Residence in or travel to areas where widespread community transmission has been reported (e.g., China, South Korea, most of Europe [including Italy], Iran, Japan).
- Potential exposure through attendance at events or spending time in specific settings where COVID-19 cases have been reported.
- The possibility of COVID-19 should also be considered in patients with severe lower respiratory tract illness when an alternative etiology cannot be identified, even if there has been no clear exposure.
2. When COVID-19 is suspected, infection control measures should be implemented and public health officials notified. Patients who do not need emergent care should be encouraged to call prior to presenting to a health care facility for evaluation. Many patients can be evaluated regarding the need for testing over the phone.
The CDC notes that the decision to test for SARS-CoV-2 should be based on clinical judgment. Most patients with confirmed COVID-19 have fever (subjective or confirmed) and/or symptoms of acute respiratory illness (e.g., cough, dyspnea). 3. In areas where testing capacity is limited, public health officials can guide prioritization of testing. The CDC suggests prioritizing testing to include hospitalized patients for infection control decisions, symptomatic individuals who have a higher risk of poor outcomes (e.g., age ≥65 years, chronic medical condition, immunocompromising conditions), and those with high exposure risk (e.g., recent travel to specific locations, contact with patients with COVID-19, or a health care worker).
Patient sampling- Several tests are currently available to test a patient for infection with this virus. Reverse Transcriptase Polymerase chain reaction (RT-PCR) tests and viral antigen tests are used to confirm cases of COVID-19 infection. Culture for the virus is not recommended. RT-PCR should be performed as soon as possible once a person has been prioritized for testing. The specimens used for testing are taken from the respiratory tract according to the patient’s clinical state:
- Nasopharyngeal swab (mild or asymptomatic suspected cases)
- Nasal swab
- Saliva
- Sputum (patients with productive cough, inducing sputum is not recommended)
- Bronchial and tracheal secretions or bronchoalveolar lavage (for patients receiving invasive mechanical ventilation)
Other laboratory tests- In patients with COVID-19, the white blood cell count can vary. Leukopenia, leukocytosis, and lymphopenia have all been reported. Lymphopenia appears most common. Elevated lactate dehydrogenase and ferritin levels are common, and elevated aminotransferase levels have also been described. High D-dimer levels and more severe lymphopenia have been associated with mortality.
Imaging findings — Chest CT in patients with COVID-19 most commonly demonstrates ground-glass opacification with or without consolidative abnormalities, consistent with viral pneumonia. Chest CT abnormalities are more likely to be bilateral, have a peripheral distribution, and involve the lower lobes.
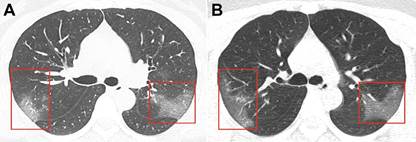
Unenhanced CT images in a 33-year-old woman. A, Image shows multiple ground-glass opacities in bilateral lungs. Ground-glass opacities are seen in the posterior segment of right upper lobe and apical posterior segment of left superior lobe. B, Image obtained 3 days after follow-up shows progressive ground-glass opacities in the posterior segment of right upper lobe and apical posterior segment of left superior lobe. The bilateralism of the peripheral lung opacities, without subpleural sparing, are common CT findings of the COVID-19 pneumonia. https://pubs.rsna.org/doi/10.1148/radiol.2020200236
Therapy and Prevention
Supportive therapy- There are currently no proven treatments for SARS CoV-2. A number are being tested and include remdesivir, chloroquine, hydroxychloroquine, favipiravir, and antibody therapies.
Mild disease; stay home, treat fever (avoid ibuprofen to reduce fever since it suppresses the immune system.), drink plenty of fluids, rest.
Severe disease; Hospitalize, supplemental oxygen, ventilation depending on need.
Prevention includes social distancing and “DO THE FIVE”- https://www.google.com/search?q=coronavirus+tips&fbx=dothefive
- Hands- wash them often.
- Elbow- cough into it.
- Face- don’t tough it.
- Feet- stay more than 3 ft apart.
- Feel- sick? Stay home.
A good video from WHO for handwashing; https://www.google.com/search?q=johns+hopkins+covid+19&rlz=1C1GGRV_enUS753US753&oq=johns+hopkins+covid+19&aqs=chrome..69i57j69i60j0.12487j0j8&sourceid=chrome&ie=UTF-8
Disinfect surfaces- bleach (diluted 1/3 cup bleach to 1 gallon of water) and ethanol (at least 70%)
Three different vaccines are approved for use in the United States- Two RNA vaccines and one viral vector vaccine. Two injections 4-6 weeks apart for primary immunization for the RNA vaccines. A booster at least 6 months after the primary immunization is recommended. The viral vector vaccine is one injection. However, some are encouraging a second injection several months later to improve protection from the virus. All three vaccines are highly effective at preventing hospitalization and deaths following infection with SARS CoV-2 (90-95%). Protection from mild to moderate illness following SARS CoV-2 infection is much lower.
Resources
General information
Coronavirus- https://www.niaid.nih.gov/diseases-conditions/coronaviruses
UptoDate- COVID-19- https://www.uptodate.com/contents/coronavirus-disease-2019-covid-19?topicRef=8298&source=see_link
UptoDate Coronaviruses- https://www.uptodate.com/contents/coronaviruses
Centers for Disease Control- https://www.cdc.gov/coronavirus/2019-ncov/about/index.html
WHO SITUATION REPORTS- https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports
EUROPEAN UNION UPDATES- https://www.ecdc.europa.eu/en/geographical-distribution-2019-ncov-cases
CDC Consumer information for coronavirus: https://www.cdc.gov/coronavirus/2019-ncov/index.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2Findex.html
CDC Healthcare Professionals information for coronavirus: https://www.cdc.gov/coronavirus/2019-ncov/hcp/index.html
CDC Clinics and healthcare facilities information for coronavirus: https://www.cdc.gov/coronavirus/2019-ncov/healthcare-facilities/index.html
COVID 19; Your Questions Answered: https://www.osmosis.org/covid-19
Transmission of COVID 19- https://www.youtube.com/watch?time_continue=127&v=G9FGrmYUr5c&feature=emb_logo
Lecturio COVID 19 article- https://www.lecturio.com/covid-19-coronavirus-disease-2019/?utm_source=lecturio-pulse&utm_medium=email&utm_campaign=covid_19_knowledge_medical_teaching_continuity_offer&utm_term=2020-03-19
Lecturio COVID-19 Video Course- https://www.lecturio.com/medical-courses/covid-19-etiology-epidemiology-diagnosis.course?utm_source=lecturio-pulse&utm_medium=email&utm_campaign=covid_19_knowledge_medical_teaching_continuity_offer&utm_term=2020-03-19#/
Interactive Maps
Interactive Covid 19 map: https://www.bing.com/covid
Johns Hopkins COVID-19 Map- https://coronavirus.jhu.edu/map.html
Social distancing and prevention
Social distancing and self quarantine; https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/coronavirus-social-distancing-and-self-quarantine
Wikipedia information on social distancing- https://en.wikipedia.org/wiki/Social_distancing
The best video explaining the math for social distancing (excellent for people who don’t like the math) https://www.facebook.com/itsokaytobesmart/videos/213119293379367/UzpfSTE1NzkxNDY5NDk6MTAyMTg2NDQyMjM4ODgzMDk/
How to hand wash with soap and water- https://www.google.com/search?q=johns+hopkins+covid+19&rlz=1C1GGRV_enUS753US753&oq=johns+hopkins+covid+19&aqs=chrome..69i57j69i60j0.12487j0j8&sourceid=chrome&ie=UTF-8
Revised 3/29/22
©2020 Neal R. Chamberlain, Ph.D., All rights reserved.