General Goal: To know the major cause(s) of these infections, how they are transmitted, and the major manifestations of the infections.
Specific Educational Objectives: The student should be able to:
1. Identify the common cause of vaginitis discussed in this handout. Know the common or pathognomonic signs of the diseases.
2. Describe the major manifestations of each infection and differentiate it from other infections in the course.
3. Describe how you diagnose, treat and prevent these infections.
Reading: MEDICAL MICROBIOLOGY by P.R. Murray, K.S. Rosenthal, G.S. Kobayashi and M.A. Pfaller, 3rd Edition. depends on the organism.
F.S. Southwick, Infectious Diseases in 30 Days, 1st edition, McGraw Hill. p. 289-318.
Lecture: Dr. Neal R. Chamberlain
References:
Polatti, F. 2012. Bacterial Vaginosis, Atopobium vaginae and Nifuratel. Current Clinical Pharmacology, 7(1):36–40. http://doi.org/10.2174/157488412799218824
VAGINITIS
Vaginal infections are the most common women's health problem, and have been increasingly linked to a growing array of serious health risks. Vaginal infections, known medically as vaginitis, are common reason for women to see their doctors. Around 10 million office visits each year. Some vaginal infections are transmitted through sexual contact (trichomoniasis), but others such as candidiasis (yeast infections) are not. Bacterial vaginosis is usually transmitted by sexual contact however; on rare occasions it can affect women who have never been sexually active. A recent Gallup survey found that very few women have a thorough understanding of vaginitis. While 95% of women surveyed had heard about yeast infections only 36 percent had ever heard of the MORE COMMON vaginal infection bacterial vaginosis (BV).
Etiology
Bacterial Vaginosis (BV) is caused by Gardnerella vaginalis, Atopobium vaginae (a gram positive rod; facultative anaerobe), Mycoplasma hominis, Ureaplasma urealyticum and various anaerobic bacteria (see below). BV is the most common vaginal infection. The disease has been found in 12 to 25 percent of women in routine clinic populations, 10 to 26 percent of women in obstetrics clinics and 32 to 64 percent of women in clinics for STI’s.
Other organisms can cause vaginitis; Candida albicans (candidiasis) and Trichomonas vaginalis (trichomoniasis). These infections of the vagina are discussed in this section as well.
Manifestations
Vaginal infections are often accompanied by vaginitis, which is an inflammation of the vagina characterized by discharge, irritation, and itching. The cause of vaginitis cannot be adequately determined solely on the basis of symptoms or a physical examination. Laboratory tests allowing microscopic evaluation of vaginal fluid are required for a correct diagnosis. A variety of effective drugs are available for treating vaginal infections and accompanying vaginitis.
Etiology
Bacterial Vaginosis (BV) is usually caused by Gardnerella vaginalis, Atopobium vaginae (a gram positive rod; facultative anaerobe), Mycoplasma hominis, Ureaplasma urealyticum and various anaerobic bacteria including Mobiluncus sp., and Prevotella sp., Prevotella sp., Porphyromonas sp., Bacteroides sp., Peptostreptococcus sp., and Fusobacterium sp.
Manifestations
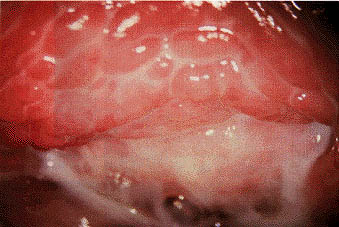
Bacterial vaginosis is usually manifested as an unpleasant vaginal odor in varying degrees and an excessive white or gray vaginal discharge with a milk-like consistency. Women often report that the odor is particularly embarrassing after sexual intercourse. When semen mixes with vaginal secretions, it lowers the acidity level to make the odor particularly strong. Odor may also be more noticeable around the time of menses. Vaginal itching or burning is sometimes present. Very little to no inflammation of the vaginal wall is observed. Up to 40% of women with BV may experience no outward symptoms. The other causes of vaginal infections, Candida albicans and Trichomonas vaginalis, cause the host to mount an inflammatory response in the vaginal wall that can be observed during gynecological exam.
BV has been associated with pelvic inflammatory disease, which can result in infertility, as well as increased risk of endometritis, cervicitis, pregnancy complications, and post-operative infections. Pregnant women with BV in the 23rd to 26th weeks of pregnancy were 40% more likely to deliver a low birth-weight baby (i.e., less than 5.5 lbs).
Epidemiology
Bacterial vaginosis (BV) is the most common cause of vaginal symptoms among women of childbearing age.
BV is associated with having multiple sex partners, a new sex partner, douching, and lack of vaginal lactobacilli.
Women who have never been sexually active are rarely affected.
Treatment of male sex partners has not been beneficial in preventing the recurrence of BV.
Pathogenesis
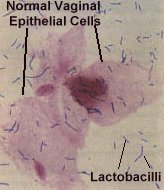
Bacterial vaginosis is caused by an overgrowth of bacteria rather than yeast. These organisms include various anaerobic bacteria, Gardnerella vaginalis, Atopobium vaginae, and Mycoplasma hominis. All of these organisms are kept to low numbers in the healthy vaginal microflora by Lactobacilli sp. In women with BV, the vaginal balance is disrupted so that these bacteria overgrow at the expense of the protective bacteria; Lactobacillus. Lactobacilli produce hydrogen peroxide to maintain a healthy and normal balance of microorganisms in the vaginal mucosa. Women who have been diagnosed with BV have up to 1,000 times more anaerobic bacteria than women without the disease. Instead of the normal predominance of Lactobacillus bacteria, increased numbers of organisms such as Gardnerella vaginalis, Atopobium vaginae, various anaerobes and Mycoplasma hominis are found in the vagina in women with BV. The cause of this imbalance in the microflora of the vaginal mucosa is not currently known. Some studies have suggested that douching may be one cause of BV.
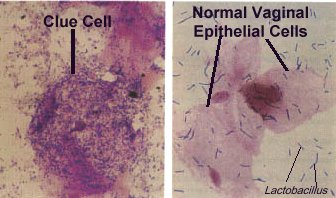
Overgrowth of Gardnerella vaginalis and other resident anaerobes only partially explains how BV develops. As these organisms overgrow and suppress the lactobacilli they also form a dense bacterial biofilm adherent to the vaginal mucosa. Clue cells one of the four diagnostic criteria used to aid in diagnosing a patient with BV are vaginal epithelial cells that are covered with this biofilm. It is the bacterial biofilm on the surface of the epithelial cells that give the clue cells their rough edge.
The biofilm formed by Gardnerella vaginalis et al., in BV is dense and strongly adherent to the vaginal epithelium. The bacterial cells in the biofilm are packed inside a network of polysaccharide fibrils. This dense bacterial biofilm coats at least half the epithelial surface, in 90% of biopsies from women with BV. Healthy women have a lot less biofilm coating the epithelial cells. Only 10% of biopsies in healthy women have evidence of biofilm coating the epithelial cells.
There are several bacteria in the biofilm besides Gardnerella vaginalis. One of increasing interest is a gram positive facultative anaerobic rod called Atopobium vaginae. In symptomatic BV it has been detected together with Gardnerella vaginalis. The bacterial composition and organization of the biofilm was examined. Gardnerella vaginalis made up 60-95% of the film mass. Atopobium vaginae accounted for 1-40% of the film mass and Lactobacillus made up only 5% of the mass of the biofilm.
Atopobium vaginae is at very low concentrations in the vaginal fluid of healthy women vaginal fluid. However, Atopobium vaginae is commonly found in the vaginal fluid of patients with BV (50%-95%). The presence of the biofilm enables the bacterial cells to reach higher concentrations (up to 1011 bacteria/mL) than in vaginal fluid and boosts their resistance to both the host immune system and the antimicrobials. It requires higher concentrations of antimicrobial agent to kill the organisms in these biofilms. It has also been shown that Atopobium vaginae is quite resistant to drugs commonly used to treat BV (metronidazole). This might explain why there is a high rate of relapse following treatment of BV.
Diagnosis
Three of four criteria should be positive to obtain a diagnosis of BV
Thin homogeneous discharge.
pH of discharge >4.5.
Clue cells in saline wet mount or Gram stain of vaginal discharge.
Mixture of vaginal discharge and 10% KOH liberates an "amine-like" or "fishy" odor.
Treatment and Prevention
Products like douches or deodorant sprays that mask vaginal odor should not be used to treat BV. Although they may temporarily eliminate odor, they will not cure the condition. It is important to tell the patient not to douche or use a feminine hygiene spray for a few days before their appointment. These products may actually hide important clues that can help in diagnosing BV, and may make the condition worse. If the patient has BV then it can be treated with the following: metronidazole or clindamycin
MYCOTIC VULVOVAGINITIS OR VULVOVAGINAL CANDIDIASIS
Etiology
The causative agent of this disease is Candida albicans.
Manifestations
The vaginal discharge frequently appears as a thick, curd like discharge containing epithelial cells and masses of hyphae/pseudohypha. The patient usually has intense pruritus of the vulva and erythematous vagina and labia. They may mention pain after urination associated with the vulva and around the urethral opening (external dysuria) that is NOT associated with increases in urinary urgency or frequency.
Epidemiology
C albicans is the second most common cause of vaginitis.
Pathogenesis
When the delicate balance of organisms in the vagina is upset, the yeast can overgrow and cause vaginitis. When a woman takes certain antibiotics to treat a bacterial infection, the antibiotic may also kill the lactobacilli that produce hydrogen peroxide to protect against yeast overgrowth. Other factors that may upset the balance and lead to yeast infection include pregnancy, obesity, diabetes, birth control pills, steroids, and prolonged exposure to moisture, and poor feminine hygiene.
Diagnosis
Diagnosis is frequently made based on the character of the vaginal discharge (i.e., curd-like discharge) and on other patient signs and symptoms. Grams stains and KOH treatment of the discharge can be performed to look for yeast cells and pseudohyphae.
Treatment and Prevention
Intravaginal agents like miconazole vaginal suppository or clotrimazole vaginal tablet can be given. An oral antifungal agent fluconazole can also be given to treat this disease.
Etiology
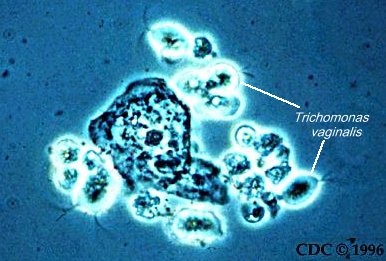
The etiological agent is a flagellated protozoan Trichomonas vaginalis. It is a pear shaped organism exhibiting a characteristic motility described as a wobbling and rotating motion, recognition of this on wet mounts is important in diagnosis.
Manifestations
In females’ proliferation of the organisms is associated with a low-grade inflammation manifested by: vulvar erythema, itching and burning, a frothy, green, creamy vaginal discharge (described as being leukorrheic and very malodorous) and dysparuenia. Because of the ease of anatomic spread to the urethra, urethritis develops and is manifested chiefly by; dysuria or increased urinary frequency. Many women with this infection may not have any symptoms.
In males’ symptoms can be associated with urethritis, prostatitis, or epididymitis however men are usually asymptomatic
.
Epidemiology
T vaginalis is a common parasite of both males and females and the incidence is in part related to hygiene.
Sexual intercourse is the usual method of transmission, especially via asymptomatic males.
In rare instances it may be passed on by wet towels, washcloths and bathing suits.
The infection often persists because the parasite rarely causes symptoms in men, so that reinfection of women by untreated men is common.
Some women can be infected for months to years as the infection is passed back and forth between the woman and her sexual partner.
For this reason, both sexual partners must be treated at the same time, even if they are in a monogamous relationship.
Pathogenesis
Low-grade inflammation is associated with the presence of high numbers of trichomonads. This parasite attaches to the cells that line the surface of the vagina and produce proteases and cytotoxic toxins that cause the host cells to round up and detach. This damage results in an immunological response from the host with many PMN’s arriving at the mucosal surface of the vagina and in the vaginal discharge. These high numbers of trichomonads become established oftentimes because of a disruption of the normal flora that has allowed them to overgrow. Immunity to infection does occur but it is only partially protective against subsequent T vaginalis infections.
Diagnosis
Clinical diagnosis depends upon recognition of the symptoms of dysuria, frothy, cream, malodorous discharges associated with punctate lesions and hyperemia of the vagina. The most practical method of specific diagnosis is microscopic examination for motile trichomonads in vaginal or urethral discharges. This vaginal discharge contains many PMN’s which usually are not present in the other causes of vaginitis.
Treatment and Prevention
Metronidazole is effective in treating this infection. Most men have asymptomatic T vaginalis infections and so can give this parasite back to their female sexual partner. The use of male condoms can lower chances of transmission from an asymptomatic male to their female sexual partner. However, the best means of avoiding reinfection is to treat the male sexual partner with metronidazole.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
"whiff" test |
|
|
|
|
| Microscopic |
epithelial cells |
|
|
|
Genitourinary Tract Infections
Return to Syllabus
Send comments and mail to Dr. Neal R. Chamberlain, nchamberlain@atsu.edu
Revised 9/30/16
©2016 Neal R. Chamberlain, Ph.D., All rights reserved.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}