MM 319-330; ID 465-485
BURULI ULCERS
NAME OF DISEASE:
Buruli ulcers, Mycoburuli ulvers
ETIOLOGICAL AGENT:
Mycobacterium ulcerans.
It grows only at temperatures below 37° C, is non-chromogenic and niacin-negative
and extracellular
Gram-positive rod.
OVERVIEW:
An ulcer of the skin and underlying tissue is the sole symptom due to the unique temperature requirements of the organism. The disease is most common along the Nile River but is also found in Southeast Asia, Australia and Mexico.
PATHOGENESIS:
The organism can apparently penetrate the unbroken skin where it produces an ulcer. Despite extensive necrosis, lesions are painless, symptoms of systemic disease are absent and there is little histological evidence of an initial acute inflammatory response. Cell replication is inhibited in the G0 G1 stage of the life cycle. Focal necrosis extends through the dermis and adipose tissue and into muscle. The cause of this necrosis is mycolactone.
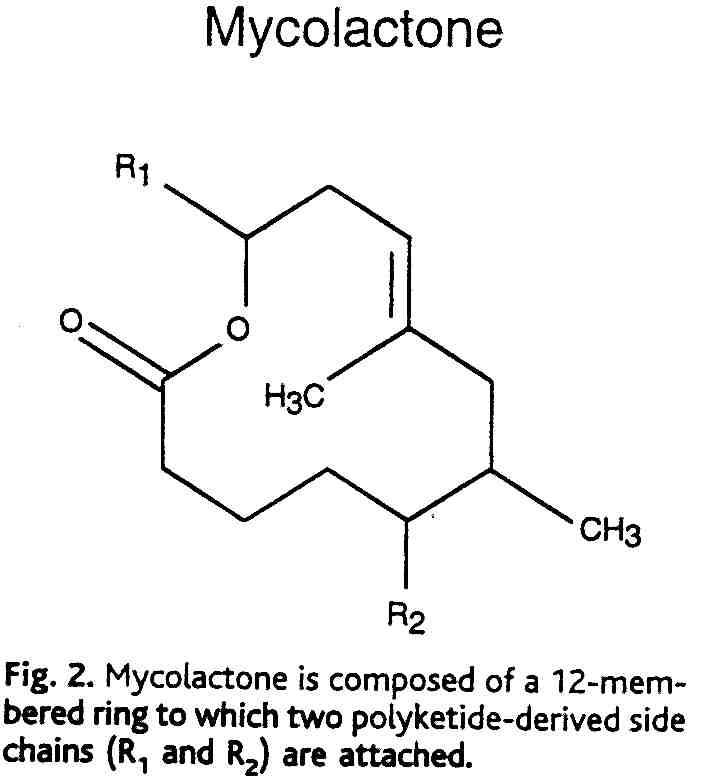
Mycolactone is the first
complex polyketide isolated from a pathogenic mycobacteria species. The
discovery that M. ulcerans toxin is a polyketide is highly significant.
Polyketides are lipid-like molecules that, although relatively small compared
with protein toxins, have potent biological activities. Well-known polyketides
include antibiotics (erythromycin), immunosuppressants (rapamycin), antifungal
agents (amphotericin B), antihelinetic agents (avermectin) and cytostatins
(bafilomycin).
DIAGNOSIS:
The presence of acid-fast,
non-niacin excreting organisms in the ulcer is diagnostic. The patient
will also give a positive tuberculin reaction.
TREATMENT:
Rifampin + amikacin or ethambutol
+ trimethoprim/sulfamethoxazole