General Goal:To know the major cause(s) of these
diseases, how they are transmitted, and the major manifestations of the
diseases.
Specific Educational Objectives: The student
should be able to:
1. identify the common cause of each of the STD's discussed in
this handout and the next two STD handouts. Know the common or pathognomonic
signs of the diseases.
2. describe the major manifestations of each disease and
differentiate it from other diseases in the course.
2. use serology in diagnosing syphilis. You should be familiar
with the pathogenesis of syphilis. You do not have to know all the information
in the handout about neurosyphilis.
3. describe how you diagnose, treat and prevent these
infections.
Reading: MEDICAL MICROBIOLOGY by P.R. Murray, K.S.
Rosenthal, G.S. Kobayashi and M.A. Pfaller, 3rd Edition. depends on the
organism.
F.S. Southwick, Infectious Diseases in 30 Days, 1st
edition, McGraw Hill. p. 289-318.
Lecture: Dr. Neal R. Chamberlain
References:
Burstein GR, Zenilman JM. Nongonococcal urethritis--a new paradigm.
Clin Infect Dis 1999 Jan;28 Suppl 1:S66-73
Hoeprich, PD., MC. Jordan, and AR. Ronald. Infectious Diseases: A Treatise
of Infectious Processes. 5th edition. 1994. J.B. Lippincott Company,
Philadelphia, PA.
CDC. The national plan to eliminate syphilis from the United States.
Atlanta, Georgia: US Department of Health and Human Services, CDC, National
Center for HIV, STD, and TB Prevention, 1999:1--84.
Sexually transmitted diseases (STD's) are among the
most common infectious diseases in the United States today. More than 20
STD's have now been identified, and they affect more than 13 million men
and women in this country each year. The annual comprehensive cost of STD's
in the United States is estimated to be well in excess of $10 billion.
It is important to understand at least five key points about all STD's
in this country today:
1. STD's affect men and women of all backgrounds and economic levels.
They are most prevalent among teenagers and young adults. Nearly two-thirds
of all STD's occur in people younger than 25 years of age.
2. The incidence of STD's is rising, in part because in the last few
decades, young people have become sexually active earlier yet are marrying
later. In addition, divorce is more common. The net result is that sexually
active people are more likely to have multiple sex partners and are more
likely to acquire STD's.
3. Usually STD's cause no symptoms. This is especially true in women.
If symptoms develop, they may be confused with those of other diseases
not transmitted through sexual contact. Even when an STD causes no symptoms
a person who is infected may be able to pass the disease on to a sex partner
(ex. genital herpes, HIV).
4. Health problems caused by STD's tend to be more severe and more frequent
for women than for men. This is because of the increased frequency of asymptomatic
infections. As a result many women do not seek care until serious problems
develop.
Some STD's can spread into the uterus and fallopian tubes to cause
pelvic inflammatory disease (PID), which in turn is the major cause of
both involuntary infertility and ectopic (tubal) pregnancy.
STD's in women also may be associated with cervical cancer (e.g. Papillomavirus
infections).
STD's can be passed from a mother to her baby before, during, or immediately
after birth. Some of these infections of the newborn can be cured easily
(ex. opthalmia neonatorium), but others may cause a baby to be permanently
disabled (ex. congenital syphilis or CMV) or even die (e.g. Herpes Simplex
virus, HIV).
5. When diagnosed and treated early, many STDs can be treated effectively.
Some infections have become resistant to the drugs used to treat them and
now require different types of antibiotics. Some can not be cured and can
be terminal (ex. HIV, chronic HBV). Experts believe that having STD's other
than AIDS increases one's risk for becoming infected with the HIV.
The prevention and control of STDs is based on the following five major
concepts:
education and counseling of persons at risk on ways to adopt
safer sexual behavior;
identification of asymptomatically infected persons and of
symptomatic persons unlikely to seek diagnostic and treatment services;
effective diagnosis and treatment of infected persons;
evaluation, treatment, and counseling of sex partners of
persons who are infected with an STD; and
preexposure vaccination of persons at risk for
vaccine-preventable STDs (Hep A and B)
Prevention of STDs begins with changing the sexual behaviors
that place persons at risk for infection. Since STD control activities reduce
the likelihood of transmission to sex partners, treatment of infected persons
constitutes primary prevention of spread within the community.
Sexual Transmission
The most reliable way to avoid transmission of STDs is to abstain from sexual
intercourse (i.e., oral, vaginal, or anal sex) or to be in a long-term, mutually
monogamous relationship with an uninfected partner. Counseling that encourages
abstinence from sexual intercourse is essential for patients who are
being treated for an STD or whose partners are undergoing treatment and for
persons who wish to avoid the possible consequences of sexual intercourse (e.g.,
STD/HIV and unintended pregnancy).
If two people wish to become sexually active the following can lower the
chances a person will acquire a STD.
Test both partners for STDs, including HIV, before initiating sexual
intercourse.
If a person chooses to have sexual intercourse with a partner whose
infection status is unknown or who is infected with HIV or another STD, a
new condom should be used for each act of insertive intercourse.
Preexposure Vaccination
Preexposure vaccination is one of the most effective methods for preventing
transmission of Hepatitis A and B infections. Hepatitis B virus infection
frequently is sexually transmitted, hepatitis B vaccination is recommended for
all unvaccinated persons being evaluated for an STD. In addition, hepatitis A
vaccine is currently licensed and is recommended for men who have sex with men (MSM)
and illegal drug users (both injection and non-injection).
Prevention Methods
Male Condom
When condoms are used consistently and correctly, they are effective in
preventing the sexual transmission of HIV infection and can reduce the risk for
other STDs (i.e., gonorrhea, chlamydia, and trichomoniasis). Since, condoms do
not cover all exposed areas, they are more effective in preventing infections
transmitted by fluids from mucosal surfaces (e.g., gonorrhea, chlamydia,
trichomoniasis, and HIV) than in preventing those transmitted by skin-to-skin
contact (e.g., herpes simplex virus [HSV], HPV, syphilis, and chancroid).
Female Condoms
Laboratory studies indicate that the female condom is an effective mechanical
barrier to viruses, including HIV. If used consistently and correctly, the
female condom may substantially reduce the risk for STDs. When a male condom
cannot be used properly, sex partners should consider using a female condom.
Vaginal Spermicides, Sponges, and Diaphragms
Recent evidence has indicated that vaginal spermicides containing nonoxynol-9
(N-9) are not effective in preventing cervical gonorrhea, chlamydia, or HIV
infection. Frequent use of spermicides containing N-9 has resulted in genital
lesions, which may be associated with an increased risk of HIV transmission.
Spermicides alone are not recommended for STD/HIV prevention.
The vaginal contraceptive sponge appears to protect against cervical
gonorrhea and chlamydia, but its use increases the risk for candidiasis.
Diaphragm use has been demonstrated to protect against cervical gonorrhea,
chlamydia, and trichomoniasis. Neither vaginal sponges nor diaphragms should be
relied on to protect women against HIV infection. Diaphragm and spermicides have
been associated with an increased risk of bacterial urinary tract infection in
women.
Condoms and N-9 Vaginal Spermicides
Condoms lubricated with spermicides are no more effective than other
lubricated condoms in protecting against the transmission of HIV and other STDs.
Rectal Use of N-9 Spermicides
Recent studies have demonstrated that N-9 may increase the risk of HIV
transmission during vaginal intercourse. Although similar studies have not been
conducted among men who use N-9 spermicide during anal intercourse with other
men, N-9 can damage the cells lining the rectum, thus providing a portal of
entry for HIV and other sexually transmissible agents. Therefore, N-9 should not
be used as a microbicide or lubricant during anal intercourse.
Nonbarrier Contraception, Surgical Sterilization, and
Hysterectomy
Women who are not at risk for pregnancy might incorrectly perceive themselves
to be at no risk for STDs, including HIV infection. Contraceptive methods that
are not mechanical or chemical barriers offer no protection against HIV or other
STDs.
The STD's will be divided into 5 different groups based on their clinical
presentations:
Diseases Characterized by Genital Ulcers
Diseases Characterized by Urethritis and Cervicitis
Diseases Characterized by Vaginal Discharge
Other STD's
Pelvic inflammatory Disease
Genital Warts (Human Papillomavirus Infections)
Epididymitis
Proctitis, Proctocolitis, and Enteritis
Ectoparasitic Infections
I. Gonorrhea
I. Gonorrhea is a sexually transmitted disease
involving infection of columnar and transitional epithelium by Neisseria
gonorrhoeae.
A. Important characteristics of
N. gonorrhoeae:
Gonococci are small Gram-diplococci
which characteristically have flattened surfaces between the adjacent individual
cocci.
Major virulence mechanisms:
Pili are small hair-like protein projections from
the cell which are important as adherence structures.
Production of an IgAase.
Ability to scavenge iron.
LPS is important.
Gonococci are very fragile and fastidious organisms;
this is important for three reasons:
They are not transmitted by fomites because they
die rapidly in the outside environment.
You should use calcium alginate swabs to collect
clinical samples because unsaturated fatty acids present in regular cotton
swabs will inhibit gonococci.
Gonococci are usually isolated on Thayer Martin medium
(chocolate agar with added Vancomycin, Colistin and Nystatin) or New York
City medium (a translucent selective medium containing V, C, N, and trimethoprim).
Gonococci generally have little tendency to develop
resistance to antibiotics but the emergence of plasmid-directed penicillinase-producing
N.
gonorrhoeae stains is an important exception; we refer to these as
PPNG.
B. Epidemiology
Man is the only known host and infection is almost
always via sexual contact.
There are about 300,000-500,000 reported cases/year
in the U.S.(45th week of 2000 there have been 293,917 cases). However since
a number of these infections are asymptomatic or not reported it is estimated
that there are 1-2 x 106 total cases/year in the U.S..
The risk of contracting gonorrhea via conventional
intercourse is 50% for women and about 20% for men following a single exposure.
C. Manifestations of gonorrhea
1. Gonococcal infection in heterosexual men usually
involves only the urethra. It causes approximately 1/3 of all cases of
urethritis in U.S.. Males with gonorrhea present with profuse purulent
urethral discharge and associated dysuria.
Following an incubation period of 2-7 days, symptoms
include:
inflammation and erythema around the opening
of the urethra
Symptomatic men generally seek treatment so the disease
does not progress; some men remain asymptomatic, however, or they ignore
early manifestations and thus are open to further complications including:
inguinal lymphadenitis
urethral stricture
local abscess formation and inflammation of neighboring
structures (epididymitis, prostatitis)
2. In homosexual men, infection involves the urethra,
anal canal, and pharynx.
Anorectal infection is manifested by:
rectal pain
mucopurulent rectal discharge
Pharyngeal infection is important as a cause of sore
throat due to pharyngitis, tonsillitis and/or gingivitis; also it is the
principal origin of gonococcemia.
3. In females gonorrhea is completely asymptomatic
approximately 30% of the time; many other cases present with only vague,
nonspecific symptoms so the women do not seek treatment.
The usual site of infection is the cervix, and this
is manifested by signs of regional inflammation (cervicitis; image
1 and image 2).
Infection of the cervix frequently leads to contiguous
spread along mucous membranes to the urethral and anal areas resulting
in:
anorectal infection manifested by pain, purulent
discharges, and rectal bleeding
urethral infection manifested by purulent exudates,
dysuria and increased frequency
bartholinitis
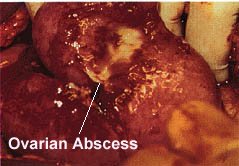
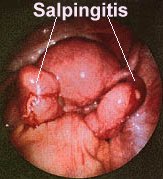
About 10-20% of cervical infections result in gonococcal
pelvic inflammatory disease (PID) due to upward spread of the bacteria
resulting in endometritis, salpingitis, tubovarian abscesses; image
1 and image 2, pelvic peritonitis and
other local complications. PID will be discussed later.
The Fitz-Hugh-Curtis
syndrome is a form of perihepatitis resulting from direct inoculation of
gonococci on the surface of the liver.
4. Disseminated gonococcal infections result in about
1-3% of cases and typically these patients are asymptomatic relative to
urogenital and/or pharyngeal infection; manifestations include:
Low grade fever
Migratory polyarthralgias involving the large joints;
septic arthritis
Increased pain and swelling
Purulent synovial fluids
Joint destruction
Tenosynovitis
Skin rashes
5. Gonorrhea in children and infants
During childbirth, gonococci infect the conjunctivitis,
pharynx, respiratory tract and gastrointestinal tract of the body.
Routine prophylaxis with 1% AgNO4
or 0.5%
erythromycin or 1% tetracycline applied directly to the eye following birth
prevents ophthalmia neonatorum.
D. Pathogenesis:
The pathogenesis of gonorrhea is related to the
ability of gonococci to attach to mucosal cells via their pili, then penetrate
to submucosal areas to induce a strong PMN cell influx.
E. Diagnosis
Diagnosis of gonorrhea involves a three-fold approach
including:
evaluation of the presenting symptoms and sexual
history;
gram stain of urethral exudates; and
culturing for N. gonorrhoeae.
Specimens are taken with calcium alginate swabs.
Specimens are plated on selective media (Thayer Martin
medium and/or New York City medium).
Urethral exudates are smeared on glass slides, stained
by Gram stain and then viewed. Three results are possible:
It is positive for gonorrhea if Gm(-) diplococci
are seen within PMNs.
It is questionable if only extracellular Gram(-)
diplococci are seen.
It is negative if no Gram(-) diplococci are seen.
F. Therapy
The drugs of choice for uncomplicated cases of
cervicitis, pharyngitis, urethritis, and proctitis are:
Cefixime 400 mg orally in a single dose, OR
Ceftriaxone 125 mg IM in a single dose, OR
Ciprofloxacin 500 mg orally in a single dose,§§ OR
Ofloxacin 400 mg orally in a single dose,§§ OR
Levofloxacin 250 mg orally in a single dose,§§ PLUS,
IF CHLAMYDIAL INFECTION IS NOT RULED OUT
Azithromycin 1 g orally in a single dose OR
Doxycycline 100 mg orally twice a day for 7 days.
1. Vaccines, most of which are composed of gonococcal
pili, were not protective.
2. Control rests on better education, proper reporting,
follow-up of patients and their contacts, use of condoms, and chemoprophylaxis
to prevent neonatal gonoccocal conjunctivitis.
II. Pelvic inflammatory disease
(PID)
II. Pelvic inflammatory disease (PID) is a disease of women defined
as the clinical syndrome resulting from the ascending
spread of microorganisms from the vagina and endocervix to the endometrium,
the fallopian tubes and/or to contiguous structures.
PID is caused by more than one organism. May include endometritis, salpingitis,
tuba-ovarian abscess, and pelvic peritonitis.
A. Etiology
N. gonorrhoeae most common
C. trachomatis most common- there are 4-8 million chlamydial infections
per year in the U.S. (number includes men and women; week 45 of 2000 there
have been 561,649 reported cases. not all cases result in PID.)
Anaerobic bacteria (ex. Bacteroides)
Facultative Gram negative rods (ex. E. coli)
Mycoplasma hominis
Actinomyces israelii (often seen in women with long-standing intrauterine
devices (IUD).
B. Pathogenesis
The exact events taking place are as yet unclear, however, it is believed
that:
prior infections of the fallopian tubes (usually of N. gonorrhoeae
or C. trachomatis) take place resulting in damage to the ciliary
cells lining the fallopian tubes;
another infection ensues and the organisms are able to ascend the fallopian
tubes and cause infections in contiguous structures.
C. Epidemiology
1. The morbidity produced by PID is greater than that of any other serious
infection. In the U.S. about 850,000 women, requiring more than 212,000
hospital admissions and 115,000 surgical procedures are reported each year.
2. Risk factors include:
Multiple sex partners
History of previous PID
Menstruation.
IUD use (oral contraceptives however decrease the risk)
Marital status (single women are at higher risk)
Asymptomatic gonococcal infection in either sexual partner.
D. Symptoms and Signs
Moderate fever (generally above 99°F)
Bilateral lower abdominal pain that is maximal in the region of the fallopian
tubes and generally lasts no longer than 14 days.
Increased vaginal discharge
Irregular bleeding
Tenderness on cervical motion
Tender adnexal mass(es)
Purulent endocervical discharge
Nausea and vomiting
NOTE: Only about 20% of the women with PID show all these signs. These
signs are quite similar to other pathologic conditions such as appendicitis,
ectopic pregnancy, septic abortion, rupture of an ovarian cyst, pyelonephritis,
etc.
E. Sequelae
The most common cause of involuntary infertility in women.
Dissemination to liver resulting in a perihepatitis.
Fitz-Hugh-Curtis syndrome; "Violin Strings"
form between the abdominal wall and liver capsule (may occur in both gonococcal
and nongonococcal types of PID).
Tubal occlusion, scarring, and adhesions (the adhesions can result in chronic
abdominal pain).
Death due to rupture of the ovarian abscesses.
F. Diagnosis (Dx)
Definitive Dx consists of direct visualization of inflamed fallopian tube(s)
on laparoscopy, laparotomy, or biopsy evidence of salpingitis (laparoscopic
image of salpingitis)(sonograph of salpingitis).
Only a confirmed culture of a biopsy of the fallopian tube positively identifies
the etiology of salpingitis.
A presumptive Dx can be made on clinical grounds alone.
Positive Gram stain for intracellular gonococci from the cul-de-sac or
endocervix.
Elevated white blood cell count.
Elevated erythrocyte sedimentation rate.
A "recent
recommendation" is to check sexually active adolescent females twice
a year for C. trachomatis. This is due to the high prevalence (29%)
of infection with this organism.
F. Treatment
Can be treated on an outpatient basis only if their temperature is <38oC,
WBC <11,000/mm3, there is minimal evidence of peritonitis,
active bowel sounds, and they are able to tolerate oral nourishment and
treatment.
Hospitalize the patient if:
the patient fails the first set of tests in item number 1
the Dx is uncertain
surgical emergencies such as appendicitis and ectopic pregnancy must be
excluded
a pelvic abscess is suspected
severe illness precludes outpatient management e. the patient is pregnant
the patient is unable to follow or tolerate outpatient regimen
the clinical follow-up after 48-72 hours of starting antibiotics cannot
be arranged
Unfortunately, no single antibiotic will be active against all possible
pathogens.
Hospitalized patients
Parenteral Cefotetan or Cefoxitin AND doxycycline
OR Clindamycin and gentamicin.
Ambulatory therapy:
Ceftriaxone and doxycycline 14 days for both
OR Ofloxicin and metronidazole 14 days for both
G. Follow-up
Close medical follow-up is essential in PID patients due to the higher
failure rates of therapeutic regimens.
Evaluation of patient 2-3 days after start of therapy for symptomatic improvement,
drug reactions, and compliance.
Repeat exam and endocervical and rectal cultures 4-7 days after completing
therapy.
Confirmation of clinical resolution by repeating exam and endocervical
culture 4-6 weeks after completing therapy.
Sex partners should be check for STD's.
Removal of IUD (this can take place during therapy).
III. Nongonococcal urethritis (NGU)
Nongonococcal urethritis (NGU) is the most frequent cause of urethritis
in heterosexual men. 45% of the cases of gonorrhea also have NGU. A number
of organisms can cause NGU and they include:
Chlamydia trachomatis- most common
Ureaplasma urealyticum- most common
Gardnerella vaginalis
Trichomonas vaginalis
Herpes Simplex virus
and other as yet unknown organisms.
A. Important characteristics of the known cause of NGU
C. trachomatis types D-K is an obligate intracellular bacteria which
requires tissue culture to grow in the laboratory. C. trachomatis
and U. urealyticum are the major causes of NGU.
Mycoplasma genitalium
U. urealyticum is a prokaryote that lacks a cell wall and can be
cultured in the lab. However, this organism is often seen in normal individuals
and culturing the organism has questionable value in diagnosing NGU.
G. vaginalis is a rod shaped gram variable bacteria which more commonly
causes vaginitis but can on occasion cause NGU in males.
T. vaginalis is a eukaryotic parasite that will be discussed in
more detail later on this week.
B. Epidemiology
Accurate data on the overall incidence of NGU is presently not available.
Men between the ages of 15 and 30, with multiple sex partners, are most
at risk.
In the U.S. it is very likely that well in excess of 50% of the cases of
urethritis are nongonococcal.
In up to 50% of the cases of NGU no etiologic agent is found.
The incidence of NGU is highly dependent on the population being served.
In the inner city and in the homosexual population primarily you will see
gonococcal urethritis. However, in primarily heterosexual populations such
as Student Health Services or private practices up to 80-90% of the urethritis
is nongonococcal.
NGU is very unusual in monogamous relationships. Most cases occur if the
male or his partner has had one or more new partners in the preceding months.
NGU is spread almost exclusively through sexual contact involving penis
to vagina or penis to rectum contact.
C. Symptoms and Signs
Urethral inflammation that is not the result of infection with Neisseria
gonorrhoeae. Urethral inflammation may be
diagnosed by the presence of one of the following criteria (1996 case
definition):
A visible abnormal urethral discharge,
or a positive leukocyte esterase test from a male aged less than 60 years
who does not have a history of kidney disease or bladder infection, prostate
enlargement, urogenital anatomic anomaly, or recent urinary tract instrumentation,
or
microscopic evidence of urethritis (greater than or equal to 5 white blood
cells per high-power field) on a Gram stain of a urethral smear
A history of urethral discharge, pain on
urination and itch in the meatal region, or by a history of a genital infection
in a male or female partner.
D. Diagnosis
No evidence of N. gonorrhoeae infection by culture, Gram stain,
or antigen or nucleic acid detection.
Diagnosis requires demonstration of a PMN response and exclusion
of N. gonorrhoeae.
The optimal time to evaluate the patient is in the morning prior to voiding,
however examination 4 or more hours after the last urination is a useful
compromise. The whole genital region should be examined for lesions and
rashes. The inguinal lymph nodes should be palpated. Collect the first
voided urine.
Specimens from the urethra should be obtained using a endourethral swab
(calcium alginate swabs are best in that fatty acids present in cotton
swabs are lethal to N. gonorrhoeae and C. trachomatis). The
swab is then used to culture for the organisms and followed by preparation
of a gram stain or methylene blue stained slide. PMN can be counted and
the presence of intracellular diplococci can be seen if the infection is
gonococcal. Five fields are scanned and a mean of greater than 4 PMN indicates
urethritis.
The first 10 to 15 mls of the first voided urine can also be used to look
for PMNs. Centrifuge the PMN and examine the sediment for PMNs. The presence
of 15 or more PMNs in one or more fields appears to be the best cutoff.
Culture of the various organisms is appropriate in all cases except NGU
caused by U. urealyticum. Many times this organism is seen in normal
individuals and culturing U. urealyticum is of little value.
C. trachomatis requires tissue culture because it is an obligate
intracellular pathogen. One looks for inclusion bodies using specific antisera
in the tissue culture cell. Serology is not particularly useful in sexually
active patients, however, serology in patients experiencing their first
episode of urethritis is useful.
A modified Diamond media is useful for T. vaginalis. Laboratory
diagnosis for the other causes of NGU is rarely done.
CDC comment: Nongonococcal urethritis (NGU) is a clinical diagnosis of exclusion.
The syndrome may result from infection with any of
several agents. If gonorrhea and chlamydia are excluded, a clinically
compatible illness should be classified as NGU. An illness in a male that
meets the case definition of NGU and C. trachomatis infection should
be classified as chlamydia. However, for the sake of simplicity I still
consider a case of NGU caused by C. trachomatis as NGU.
E. Treatment
Doxycycline for at least 7 days OR Erythromycin for 7 days OR single treatment
with a single 1 g dose of azithromycin.
Patients should be advised to return if symptoms persist or recur.
All sex partners should be examined for STD and promptly treated.
Persistent or recurrent NGU. Look for untreated or noncompliant sex partners.
If the sex partners have been treated and complain check for less common
causes of urethritis.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}